Vivek Lingiah, MD, Mumtaz Niazi, MD Rutgers New Jersey Medical School, Newark, NJ
Introduction: Acute on Chronic Liver Failure (ACLF) is a disorder that results in grave systemic consequences. The dysregulated inflammatory response caused by an acute liver injury often results in multi-organ dysfunction. And while alcoholic/viral hepatitis or infections are common causes of ACLF, hematologic disorders are unusual. We present a case of ACLF due to sickle cell intrahepatic cholestasis from SC disease.
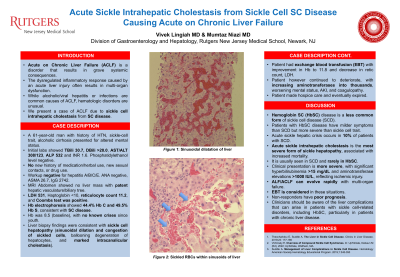
Case Description/Methods: A 61-year-old man with history of HTN, sickle-cell trait, alcoholic cirrhosis presented for altered mental status. Initial labs showed TBili 30.7, DBili >20.0, AST/ALT 308/123, ALP 532 and INR 1.6. Phosphatidylethanol level negative. No new history of medication/herbal use, new sexual contacts, or drug use. Workup negative for hepatitis A/B/C/E. ANA negative, ASMA 26.7, IgG 2742. MRI Abdomen showed no liver mass with patent hepatic vasculature/biliary tree. LDH 531, Haptoglobin < 10, reticulocyte count 11.2, and Coombs test was positive. Hb electrophoresis showed 44.4% Hb C and 49.5% Hb S, consistent with SC disease. Hb was 8.5 (baseline), with no known crises since youth. Liver biopsy findings were consistent with sickle cell hepatopathy (sinusoidal dilation and congestion of sickled cells, ballooning degeneration of hepatocytes, and marked intracanalicular cholestasis). Patient had exchange blood transfusion (EBT) with improvement in Hb to 11.8 and decrease in retic count, LDH. Patient however continued to deteriorate, with increasing aminotransferases into thousands, worsening mental status, AKI, and coagulopathy. Patient made hospice care and eventually expired.
Discussion: Hemoglobin SC (HbSC) disease is a less common form of sickle cell disease (SCD). Patients with HbSC disease have milder symptoms than SCD but more severe than sickle cell trait. Acute sickle hepatic crisis occurs in 10% of patients with SCD. Acute sickle intrahepatic cholestasis is the most severe form of sickle hepatopathy, associated with increased mortality. It is usually seen in SCD, but rarely in HbSC. Clinical presentation is more severe, with significant hyperbilirubinemia >15 mg/dL and aminotransferase elevations >1000 IU/L, reflecting ischemic injury. ALF/ACLF can evolve rapidly with multi-organ failure. EBT is considered in these situations. Non-responders have poor prognosis. Clinicians should be aware of the liver complications that can arise in patients with sickle cell-related disorders, including HbSC, particularly in patients with chronic liver disease.
Disclosures:
Vivek Lingiah indicated no relevant financial relationships.
Mumtaz Niazi indicated no relevant financial relationships.
Vivek Lingiah, MD, Mumtaz Niazi, MD. C0595 - Acute Sickle Intrahepatic Cholestasis From Sickle Cell SC Disease Causing Acute on Chronic Liver Failure, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.

.jpg "Vivek Lingiah, MD photo")