Allegheny General Hospital Pittsburgh, Pennsylvania
Bandhul Hans, MD, Pamela Kim, MD, Raghunath Appasamy, MD, PhD, Manish Dhawan, MD Allegheny General Hospital, Pittsburgh, PA
Introduction: Candy cane syndrome is an underrecognized complication of Roux-en-Y gastric bypass resulting from a long blind afferent Roux limb at the gastrojejunostomy causing nausea, vomiting, reflux and pain due to food accumulation. We present a case of novel endoscopic treatment of candy cane syndrome.
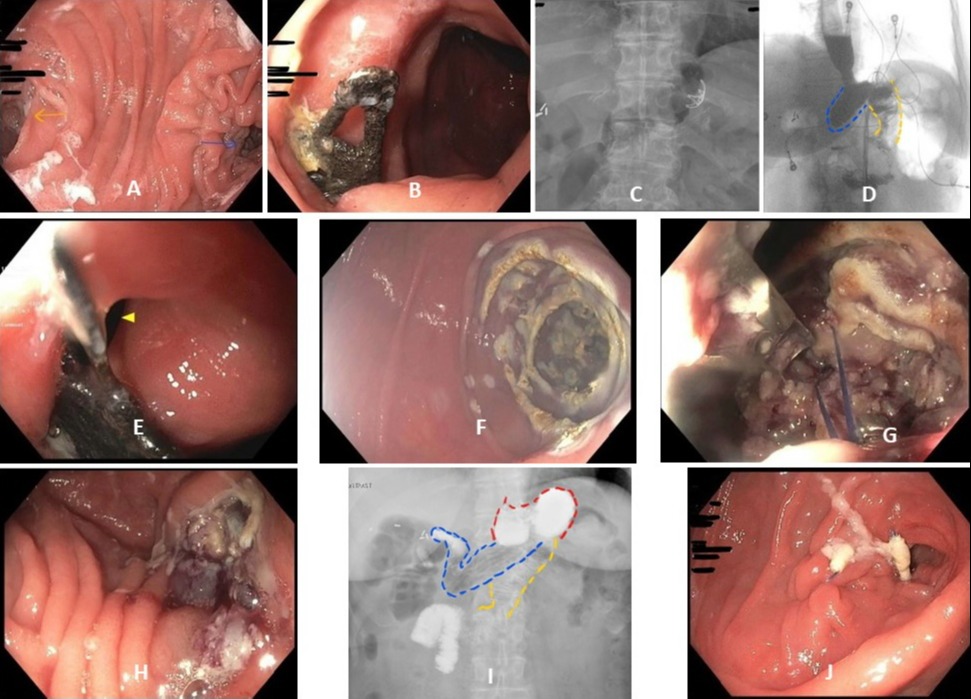
Case Description/Methods: 67-year-old female with vertical banded gastroplasty revised to Roux-en-Y gastric bypass and multiple open abdominal surgeries presented with worsening of persistent post prandial epigastric pain. Upper endoscopy showed Roux-en-Y anatomy. Also noted was gastro-gastric (GG) fistula (Pic 2A) and an embedded over the scope clip (OTSC) in this area (Pic 1B). There were no medical records of placement of the clip or patient recall of OTSC clip. A fluoroscopic upper GI series showed candy cane loop and gastro-gastric (GG) fistula (Pic 1D). Her bariatric surgeon felt that her acute symptoms were likely from candy cane syndrome. Given that she had a fairly extensive surgical history she was deemed high risk for surgery, decision made to offer endoscopic therapy for candy cane syndrome. APC (1L/min, 50W) was used to coagulate the mucosal layer of the entire afferent limb (Pic 1F) and then the enteric walls of the afferent limb were approximated by placing three purse string sutures using endoscopic suturing device attached to a 2-channel therapeutic upper endoscope (Pic 1G). Sutures started from the end of the blind limb towards the GJ anastomosis leading to total closure of the afferent limb (Pic 1H). One month follow up upper GI series showed direct transit of most of the contrast into efferent limb with redemonstration of a much smaller though persistent candy cane limb (Pic 1I and J).
Discussion: Candy cane syndrome results from creation of a long nonfunctional limb during creation of gastro-jejunostomy at time of gastric bypass. This causes intestinal dysmotility resulting in stasis, and gradual expansion of the limb over time. Upper GI series has been used traditionally to diagnose this condition though endoscopic demonstration of off-axis orientation of roux limb using a simple guide wire has also been proposed. Historically, it has been managed surgically. We present an interesting case of endoscopic reduction of candy cane loop using advanced endoscopic suturing technique.
Figure: Picture 1. (A) Roux-en-Y anatomy with afferent limb (blue), efferent limb (yellow). (B) Metallic prong seen in the lumen of gastric pouch. (C) Metallic FB identified as OTSC clip on x ray. (D) Upper GI series demonstratingrapid pooling of contrast in candy cane limb (blue) and the Roux limb (yellow). (E) fistula seen adjacent to the clip. (F) ablated afferent limb mucosa. (G) purse string suturing of the ablated afferent limb. (H) completely obliterated of afferent limb after sutures. (I) upper GI series 1 month later shows transit of most contrast from gastric pouch (red) into Roux limb (yellow) but a persistent cany cane limb (blue). (J) one month post suturing endoscopic view of closed afferent limb
Disclosures:
Bandhul Hans indicated no relevant financial relationships.
Pamela Kim indicated no relevant financial relationships.
Raghunath Appasamy indicated no relevant financial relationships.
Manish Dhawan indicated no relevant financial relationships.
Bandhul Hans, MD, Pamela Kim, MD, Raghunath Appasamy, MD, PhD, Manish Dhawan, MD. E0454 - Novel Endoscopic Technique for Treatment of Candy Cane Syndrome, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.