University of Arkansas for Medical Sciences Los Angeles, CA
Cody J. Timmermann, MD, Nimy John, MD, Camila C. Simoes, MD, Ragesh B. Thandassery, MD, DM, Matthew G. Deneke, MD, Mary Rude, MD University of Arkansas for Medical Sciences, Little Rock, AR
Introduction: Acute graft versus host disease (aGVHD) is a rare complication of orthotopic liver transplant (OLT) with estimated 75-85% mortality. GVHD is a common complication of an allogeneic bone-marrow transplant.Incidence of aGVHD in OLT is about 0.1% and presents with rash, fever, diarrhea, and pancytopenia. Diagnosis is difficult given the non-specific symptoms, overlapping infections,drug reactions in patients on immunosuppression. Mortality is associated with bone marrow failure. Early diagnosis and treatment are vital to survival. This report aims to juxtapose two cases of aGVHD after OLT. Chart review was conducted to obtain the history and progression of two patients with post-liver transplant GVHD.
Case Description/Methods: First case is a Hispanic patient who underwent OLT for decompensated HCV cirrhosis. The patient presented 3 months postop with diffuse rash. He was admitted two weeks later with worsening rash, fever, flu-like symptoms, and diarrhea. GVHD was diagnosed by skin biopsy and treated with steroids and ruxolitinib (JAK1/2 inhibitor). The patient improved, but ultimately expired six months later due to bone marrow failure and infectious complications (invasive fungal sinusitis, VRE bacteremia, clostridium difficile infection, multifocal pneumonia).
Second case is a Caucasian patient who underwent OLT for decompensated NASH cirrhosis. The patient was admitted 3 weeks postop with fever, cough, sore throat and headache. Diarrhea and rash developed shortly after and extensive infectious workup was unremarkable. aGVHD was diagnosed by skin biopsy and treated with steroids and ruxolitinib. The patient’s clinical course was complicated by pseudomonas bacteremia, abdominal surgical wound infection, ecthyma gangrenosum of his right thigh requiring surgical debridements and IV antibiotics. Despite many complications, he is living to this date (over 2.5 years from the diagnosis of GVHD) and doing well.
Discussion: Both cases of aGVHD occurred at the same center less than one month apart, but one was fatal. Both patients received MMF as part of their immunosuppression (Per studies, MMF reduces the risks of fatal GVHD). Only the second patient (who survived) received basiliximab for induction (Studies show that risks of fatal GVHD increase in association with basiliximab induction). The principal difference between the two cases is the time of symptom onset and time to treatment initiation. The patient who survived had earlier symptom onset, a rapid diagnosis, and early-onset treatment.
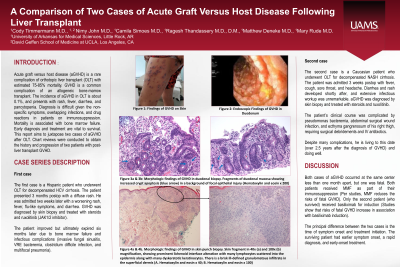
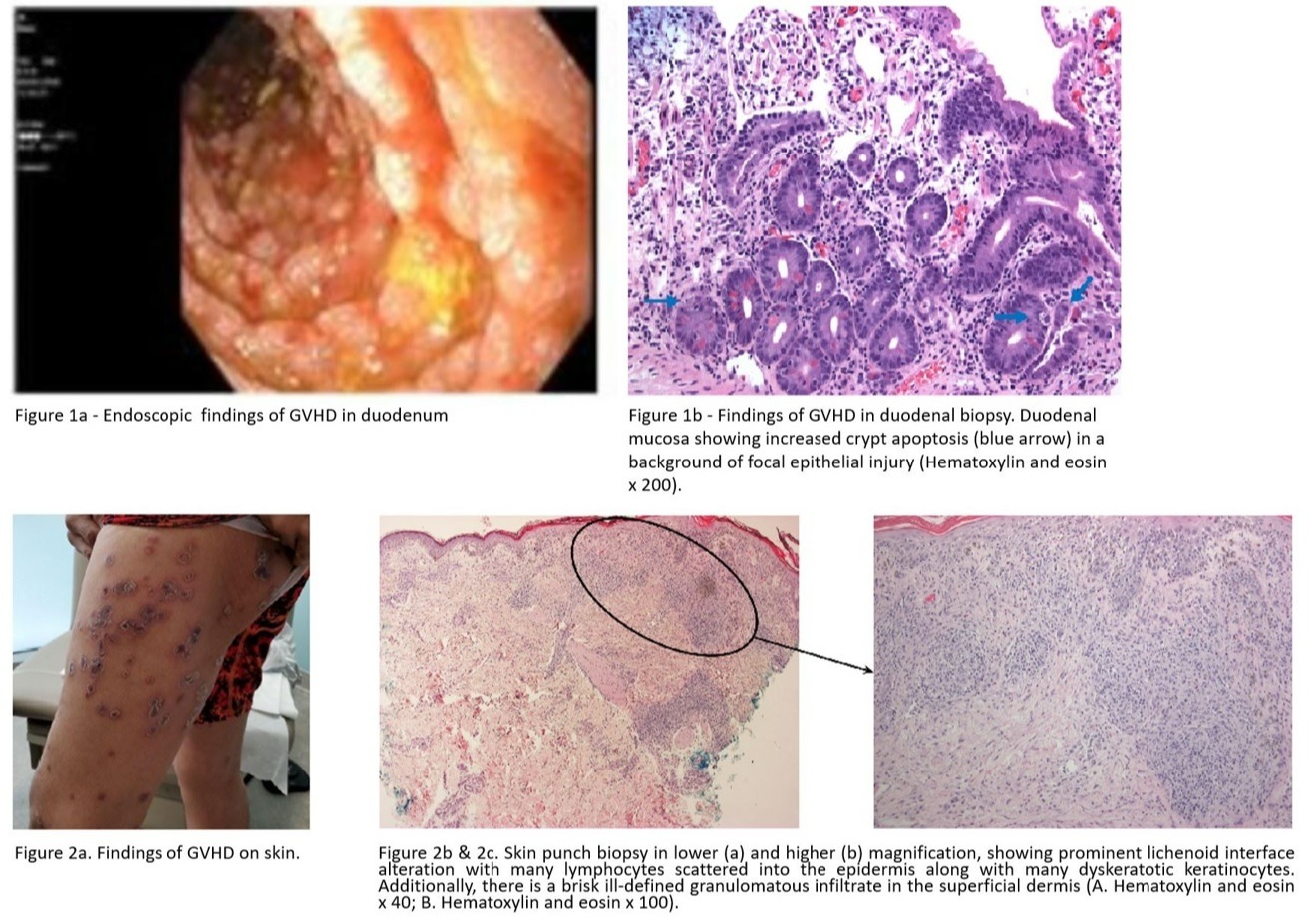
Figure: GVHD Findings
Disclosures:
Cody Timmermann indicated no relevant financial relationships.
Nimy John indicated no relevant financial relationships.
Camila Simoes indicated no relevant financial relationships.
Ragesh Thandassery indicated no relevant financial relationships.
Matthew Deneke indicated no relevant financial relationships.
Mary Rude indicated no relevant financial relationships.
Cody J. Timmermann, MD, Nimy John, MD, Camila C. Simoes, MD, Ragesh B. Thandassery, MD, DM, Matthew G. Deneke, MD, Mary Rude, MD. A0523 - A Comparison of Two Cases of Acute Graft versus Host Disease Following Liver Transplant, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.