Bishal Paudel, MD, Emily S. Edwards, MD, MS, Eric S. Sobel, MD, PhD, Amy J. Sheer, MD, MPH University of Florida, Gainesville, FL
Introduction: Sarcoidosis is a disorder characterized by the formation of non-caseating granulomas in multiple organ systems. While pulmonary manifestation is the most common presentation, hepatic involvement can be seen in many patients. Most patients with liver involvement are asymptomatic; however, some can present with symptoms of liver injury. The presentation of hepatic sarcoidosis can resemble many other disease processes. Since definite diagnostic criteria have not yet been formalized for hepatic sarcoidosis, it can often be challenging for providers to make a prompt diagnosis.
Case Description/Methods: We present the case of a 36-year-old female who was evaluated for generalized abdominal pain and left flank pain. On presentation, labs were notable for calcium at 13 mg/dl, ionized calcium at 1.62 mmol/l, PTH at 8 pg/ml,1,25-dihydoxyvitamin D at 96.4 pg/ml, alkaline phosphatase at 192 IU/L, AST at 51 IU/L and ALT at 47 IU/L.
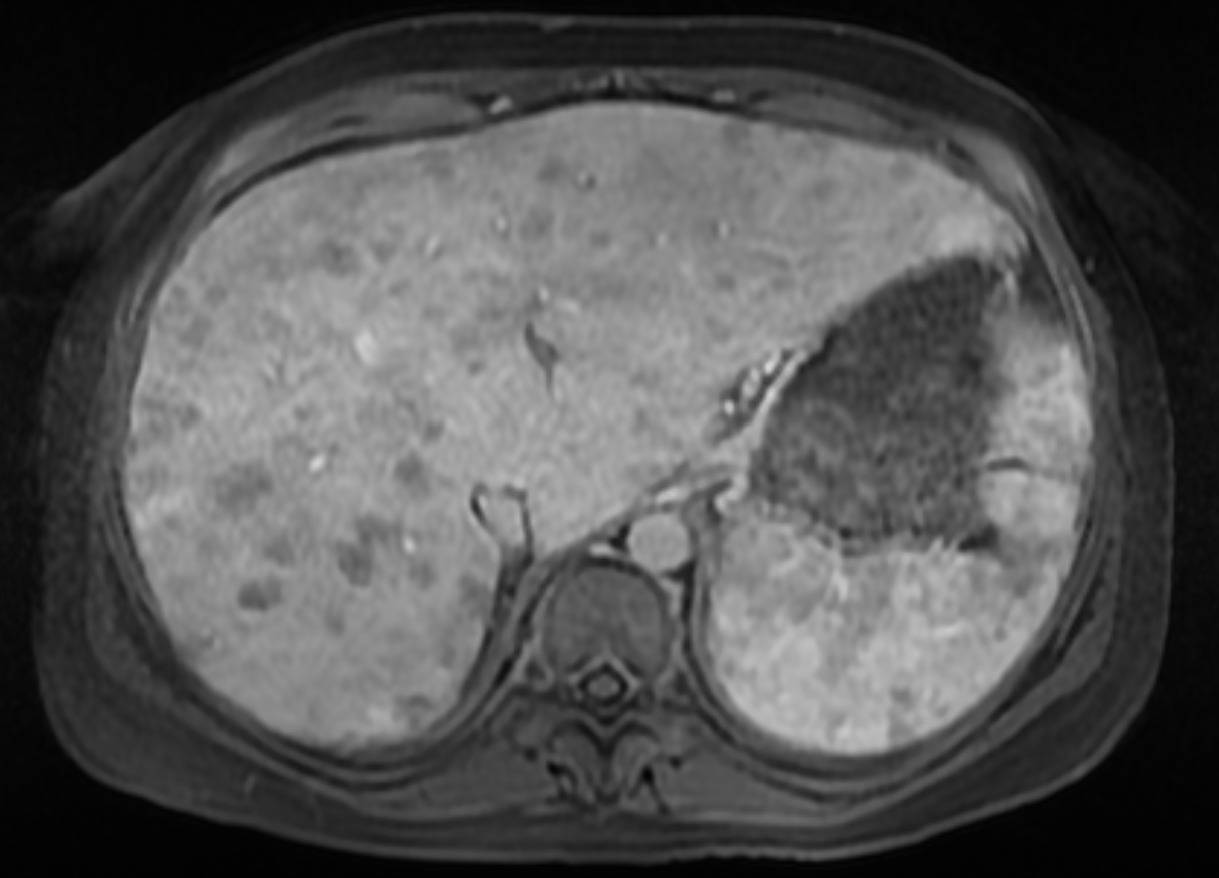
Eight months prior, the patient was admitted to an outside hospital in the setting of hematemesis. EGD with variceal banding was performed, and she was diagnosed with cryptogenic liver cirrhosis. CT A/P demonstrated marked heterogeneity of the liver. MRI of the abdomen showed mild hepatosplenomegaly and “diffuse small areas of altered signal intensity throughout the liver suspicious for diffuse hepatic metastatic disease” (Figure A). The patient just had her first visit with an oncologist prior to her presentation to our hospital.
Her physical exam was notable for hepatomegaly, abdominal distension and RUQ tenderness. Her hypercalcemia was treated with fluids. Infectious and autoimmune workup came back negative. Different tumor markers including CA 19-9, CA 27-29 and CA 125 were normal. Liver biopsy showed hepatic parenchyma with numerous non-necrotizing granulomas and associated fibrosis. IL-2R receptor-serum came back elevated at 2916.1 pg/ml. The patient was then started on 20 mg prednisone daily for treatment of hepatic sarcoidosis.
Discussion: Hepatic sarcoidosis can have a wide spectrum of clinical presentation, ranging from incidental finding to end-stage liver disease. When a patient is diagnosed with a new hepatic disease, keeping hepatic sarcoidosis on the differential is very important. In case of hepatic sarcoidosis, assessing symptoms of liver involvement and biochemical evidence of cholestasis is crucial. While observation is indicated for asymptomatic liver disease, corticosteroids and/or ursodeoxycholic acid are the first line agents for symptomatic disease.
Figure: Figure A: Hypointense liver lesions on MRI, initially presumed suspicious for diffuse hepatic metastatic disease, later confirmed to be sarcoid lesions
Disclosures:
Bishal Paudel indicated no relevant financial relationships.
Emily Edwards indicated no relevant financial relationships.
Eric Sobel indicated no relevant financial relationships.
Amy Sheer indicated no relevant financial relationships.
Bishal Paudel, MD, Emily S. Edwards, MD, MS, Eric S. Sobel, MD, PhD, Amy J. Sheer, MD, MPH. C0559 - Hepatic Sarcoidosis Presenting as Decompensated Liver Cirrhosis, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.