University of Michigan Medical Center Ann Arbor, MI
Michael W. Song, MD, Suraj Pai, MD, Fadi Hawa, MD, Jeffrey Berinstein, MD University of Michigan Medical Center, Ann Arbor, MI
Introduction: Crohn’s Disease (CD) is a chronic idiopathic inflammatory bowel disease with variable clinical and histologic manifestations. Microscopic findings include transmural inflammation and may show granuloma in a subset of patients. The impact of extraintestinal granulomatous inflammation in CD is not well understood. We present an atypical initial presentation of CD in the form of diffuse granulomatous mesenteric adenitis.
Case Description/Methods: A 31-year-old woman with ampiginous choroiditis presented with a month of diffuse abdominal pain and fever. Computed tomography (CT) of the abdomen/pelvis showed diffuse mesenteric lymph node enlargement with normal appearing bowels.
Given her fevers, lymphadenopathy, mild leukocytosis, and elevation in inflammatory markers, thorough infectious and rheumatologic workups were pursued and unrevealing. Whole body positron emission tomography showed hypermetabolic mesenteric lymph nodes and terminal ileitis; subsequent colonoscopy noted inflamed, friable mucosa with biopsies showing active ileitis, ulceration, architectural distortion, and well-formed intramucosal granuloma consistent with Crohn’s ileitis. CT-guided lymph node biopsy also showed granulomatous inflammation, making sarcoidosis a differential diagnosis.
The patient was discharged in stable condition and followed at the outpatient gastroenterology clinic. Given uncertainty regarding the underlying diagnosis, she was trialed on 2 months of budesonide. MRE following treatment showed significantly improved inflammation of the terminal ileum with resolution of mesenteric lymphadenopathy.
Discussion: Mesenteric adenitis with terminal ileitis has been shown to occur in infectious ileitis, CD, and sarcoidosis. Rarely, CD can coexist with sarcoidosis.
CD has transmural inflammation, with ulceration and granuloma formation, in contrast to intestinal sarcoidosis which only involves the mucosa. Granulomas outside the gastrointestinal tract favor the diagnosis of sarcoidosis but can still occur with CD. In CD, the location of granulomatous inflammation may play a role in predicting clinical course. The presence of mesenteric lymph node (MLN) granulomas has been associated with younger age, transmural inflammation, and postoperative disease recurrence risk.
Mesenteric granulomatous adenitis without intestinal involvement can be the initial presentation of CD, as noted in our patient. Prompt evaluation of competing diagnoses is warranted to ensure timely diagnosis and management.
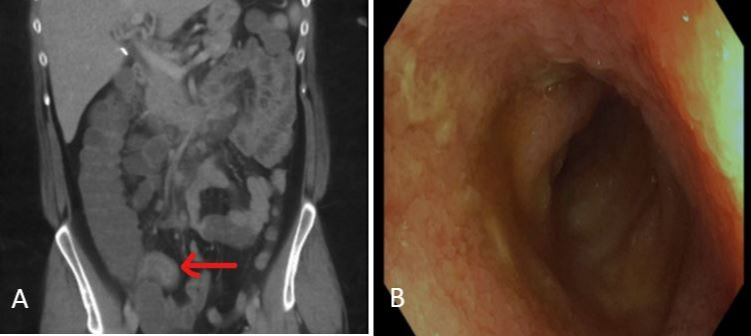
Figure: A. Computed tomography showing mesenteric haziness and terminal ileitis (red arrow). B. Endoscopic findings of inflamed terminal ileum with congested, erythematous, and ulcerated mucosa.
Disclosures:
Michael Song indicated no relevant financial relationships.
Suraj Pai indicated no relevant financial relationships.
Fadi Hawa indicated no relevant financial relationships.
Jeffrey Berinstein indicated no relevant financial relationships.
Michael W. Song, MD, Suraj Pai, MD, Fadi Hawa, MD, Jeffrey Berinstein, MD. A0413 - Crohn's Disease Presenting as Diffuse Granulomatous Mesenteric Adenitis, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.