Christopher Chhoun, DO1, Neethi Dasu, DO2, Kirti Dasu, BA3, Yaser Khalid, DO4, Drew Chiesa, DO5 1Jefferson Health NJ, Voorhees, NJ; 2Jefferson Health New Jersey, Voorhees, NJ; 3Drexel Graduate School of Biomedical Sciences and Professional Studies, Philadelphia, PA; 4Wright Center for GME/Geisinger Health System, Scranton, PA; 5Jefferson Health New Jersey, Turnersville, NJ
Introduction: Double Pylorus Syndrome or gastroduodenal fistula is a rare entity usually found incidentally on endoscopy. This syndrome can be congenital or secondary to gastric malignancy or peptic ulcer disease. The pylorus has two openings which connect the duodenal bulb to the gastric antrum. This syndrome is extremely rare and found in less than .5% of cases. Recurrent gastrointestinal (GI) bleeding can occur secondary to inadequate epithelization of the tract and recurrent ulcerative disease. We present a unique consequence of peptic ulcer disease in a 68 year old female found to have Double Pylorus Syndrome.
Case Description/Methods: A 68 year-old female with PMH of atrial fibrillation on anticoagulation presented to the hospital for evaluation of iron deficiency anemia and was found to have a hemoglobin of 6.8. She was treated with an intravenous proton pump inhibitor drip and iron supplementation. Iron studies revealed an iron level was 19 with a ferritin of 11. She had undergone prior upper endoscopic evaluation which revealed a non-bleeding gastric ulcer in the antrum. She underwent repeat esophagogastroduodenoscopy which revealed a duodenal ulcer with active oozing which was treated with epinephrine, two endoclips, and gold probe electrocautery. A double pylorus was also seen. The patient was discharged with a course of PPI therapy and was cleared to resume anticoagulation, however, she deferred restarting until discussion with her outpatient cardiologist.
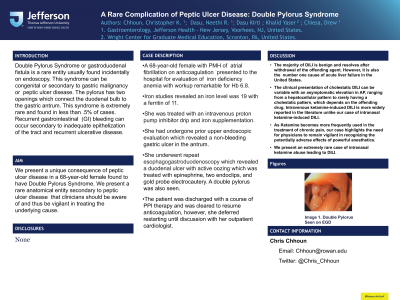
Discussion: Our case represents an acquired form of Double Pylorus Syndrome (Image 1) which is a rare complication of peptic ulcer disease. Acquired gastro-duodenal fistulas are uncommon and typically present in the prepyloric region in combination with chronic peptic ulcer disease as seen with our patient. This type of fistula forms due to inflammation of the gastric gastric antrum or duodenal bulb leading to adhesions that form between the gastric and duodenal walls. Standard treatment is with a proton pump inhibitor, avoiding triggers such as NSAIDs and corticosteroids, and eliminating H. pylori if present. Our patient responded well to medical management. Surgical intervention is necessary if there are refractory symptoms, perforation, or failure of endoscopic treatment. We present a rare anatomical entity secondary to peptic ulcer disease that clinicians should be aware of and thus be vigilant in treating the underlying cause.
Figure: Figure 1: Double Pylorus
Disclosures:
Christopher Chhoun indicated no relevant financial relationships.
Neethi Dasu indicated no relevant financial relationships.
Kirti Dasu indicated no relevant financial relationships.
Yaser Khalid indicated no relevant financial relationships.
Drew Chiesa indicated no relevant financial relationships.
Christopher Chhoun, DO1, Neethi Dasu, DO2, Kirti Dasu, BA3, Yaser Khalid, DO4, Drew Chiesa, DO5. B0700 - A Rare Complication of Peptic Ulcer Disease: Double Pylorus Syndrome, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.