Indiana University School of Medicine Indianapolis, IN
Abid Ahmad, MD, Howard Masuoka, MD, PhD, John Guardiola, MD Indiana University School of Medicine, Indianapolis, IN
Introduction: This case illustrates the complexity of diagnosis of Budd-Chiari syndrome especially with an atypical presentation.
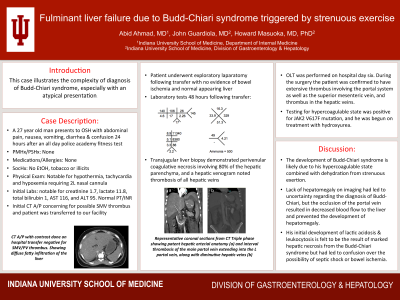
Case Description/Methods: A 27-year-old man in his usual good state of health attended an all-day police academy fitness test. That evening he developed abdominal pain, nausea, vomiting, and diarrhea. He left work the next day due to these symptoms and progressive confusion. His family called EMS and he was transported to a local emergency department where he was found to be hypothermic, tachycardic, and hypoxemic. Labs were notable for acute kidney injury with creatinine 1.7, lactate 11.8, total bilirubin 1, AST 116, and ALT 95. He was begun on 2 vasopressors and empiric antibiotics. CT Abdomen noted a possible mesenteric thrombus; he was taken emergently to the operating room, but no bowel ischemia was found. His laboratory tests increased over the next 3 days reaching total bilirubin 3.0, AST 8560, ALT 5880, alkaline phosphatase 92, albumin 2.7, creatinine 3.1, INR 5.06, WBC 34.5, and ferritin 18,724. He was subsequently transferred to a tertiary center where his mental status worsened, and he was intubated. A transjugular liver biopsy demonstrated perivenular coagulative necrosis involving 80% of the hepatic parenchyma, and a hepatic venogram noted extensive portal vein thrombus. He had no history of taking any medications on a regular basis and did not take acetaminophen. An acetaminophen level was negative. Orthotopic liver transplantation was performed on the sixth day after his initial hospital presentation. During the surgery the patient was noted to have extensive thrombus involving the portal system including the main portal vein as well as the superior mesenteric vein, and thrombus in the hepatic veins. Testing for hypercoagulable state was positive for JAK2 V617F mutation, and he was begun on treatment with hydroxyurea.
Discussion: His development of Budd-Chiari syndrome is felt to be due to this hypercoagulable state combined with dehydration from strenuous exertion. There was no hepatomegaly noted on imaging which had led to confusion regarding the diagnosis of Budd-Chiari syndrome, but the occlusion of the portal vein in this patient resulted in decreased blood flow to the liver and prevented the development of hepatomegaly. His initial development of lactic acidosis, leukocytosis, and elevated ferritin is felt to be the result of marked hepatic necrosis from the Budd-Chiari syndrome but had led to confusion over the possibility of septic shock or bowel ischemia.
Disclosures:
Abid Ahmad indicated no relevant financial relationships.
Howard Masuoka indicated no relevant financial relationships.
John Guardiola indicated no relevant financial relationships.
Abid Ahmad, MD, Howard Masuoka, MD, PhD, John Guardiola, MD. E0526 - Fulminant Liver Failure Due to Budd-Chiari Syndrome Triggered by Strenuous Exercise, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.