Wayne State University/Detroit Medical Center Detroit, MI
Sarvani Surapaneni, MD1, Katherine Wong, MD2, Jing Wang, MD1, Angy Hanna, MD1, Anirudh R. Damughatla, DO1 1Wayne State University/Detroit Medical Center, Detroit, MI; 2Detroit Medical Center, Detroit, MI
Introduction: Hemolysis, elevated liver enzymes, and low platelet count (HELLP) syndrome is seen in 0.1-1.0% of pregnant people overall, with the risk increased by preeclampsia. Common complications of HELLP include bleeding, disseminated intravascular coagulation (DIC), and abruptio placentae. Here we present a rare case of subcapsular liver hematoma that occurs in only 1% of HELLP patients.
Case Description/Methods: A 29-year-old woman, gravida 4, para 3 with a history of preeclampsia during prior pregnancies presents with acute onset epigastric and pelvic pain for one day at 27th-week gestation. The severe, intermittent epigastric pain radiates laterally down to the pelvis and is aggravated with laying down. The review of systems and vitals were normal. Mild tenderness in the right upper quadrant (RUQ) was noted. Labs showed high ALT 233 U/L, AST 378 U/L, low platelet 108,000/microL, and high LDH 519 IU/L. The rest of the labs were normal. She underwent an emergent C-section at admission for HELLP syndrome. An ultrasound showed two complex hypoechoic hepatic mass-like areas measuring 9.3cm and 3.5 cm in the setting of hepatomegaly and diffuse hepatic steatosis suggestive of focal fatty sparing or cavernous hemangioma. Biliary sludge without cholecystitis or cholelithiasis was also noted. An MRI with IV contrast with the liver mass protocol was obtained which showed hepatic subcapsular hematoma of dimensions 24 cm x 9.2 cm x 3.9 cm at the level of the right hepatic lobe. The pain continued to worsen with a drop in hemoglobin from 12.8 gm/dl at admission to 7.1 gm/dl on day 4. IR was consulted for rupture concern and recommended CT angiography of abdomen and pelvis with and without arterial/venous phase that showed similar appearing subcapsular hematoma without an active bleed. Underwent image-guided hepatic angiography that showed large perihepatic hematoma along the right lateral abdominal wall without active contrast extravasation. Right hepatic artery embolization was done with a reduction in peripheral hepatic arterial blood flow by 25%. Later hemoglobin stabilized, liver enzymes improved, and the patient was discharged home 6 days later in a clinically stable state.
Discussion: Early diagnosis of subcapsular hematoma is challenging due to nonspecific signs and symptoms but crucial for improved outcomes. Physicians should evaluate for a subcapsular hematoma in patients with HELLP and RUQ pain or hypotension. Therapeutic options for ruptured hematomas include laparotomy and hepatic artery embolization.
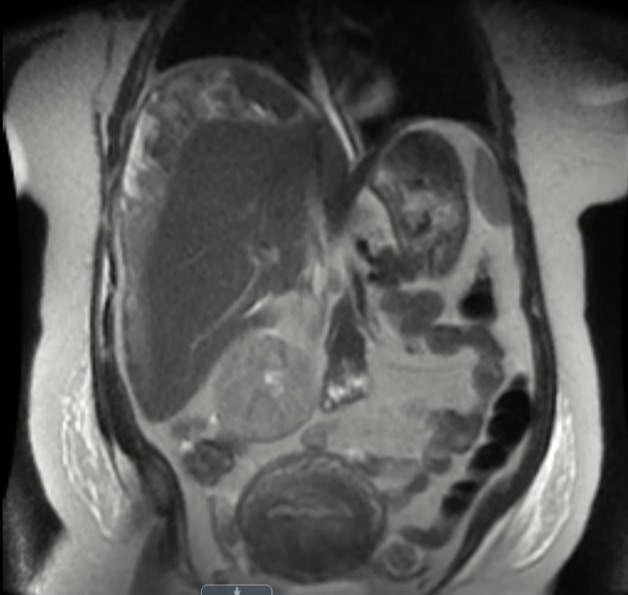
Figure: Coronal section of MRI with IV contrast (Liver mass protocol) of abdomen and pelvis demonstrates subcapsular hepatic hematoma involving the hepatic dome and right hepatic lobe approximately measuring 24 cm in craniocaudal dimension.
Disclosures:
Sarvani Surapaneni indicated no relevant financial relationships.
Katherine Wong indicated no relevant financial relationships.
Jing Wang indicated no relevant financial relationships.
Angy Hanna indicated no relevant financial relationships.
Angy Hanna — NO DISCLOSURE DATA.
Anirudh Damughatla indicated no relevant financial relationships.
Sarvani Surapaneni, MD1, Katherine Wong, MD2, Jing Wang, MD1, Angy Hanna, MD1, Anirudh R. Damughatla, DO1. E0531 - Subcapsular Hepatic Hematoma: A Rare Complication of Hemolysis, Elevated Liver Enzymes, and Low Platelet Count (HELLP) Syndrome in Pregnancy, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.