Tushar Khanna, MD1, Suhind Kodali, MD2, Christopher Hakim, MD3, Stefan Odabasic, MD1, Fadi Alali, MD3, Serge Sorser, MD3, Jay Levinson, MD3 1St. Mary Mercy Hospital, Livonia, MI; 2Ascension Providence Hospital, Southfield, MI; 3Ascension Providence Hospital - Southfield Campus, Southfield, MI
Introduction: Small cell lung cancer (SCLC) is an aggressive high grade neuroendocrine carcinoma that accounts for 15% of all lung cancers & usually presents with early distant metastatic spread typically to liver, bone, brain & lung on diagnosis. Pancreas is a very uncommon site of metastasis. We present a rare case of SCLC metastasis to the pancreas presenting as obstructive jaundice upon initial presentation.
Case Description/Methods: A 62-year-old male with a past medical history of recurrent pancreatitis presented to the emergency department with abdominal pain, nausea, vomiting, & jaundice. Routine blood work on admission were notable for elevated total bilirubin of 16.4 mg/dL along with elevation in alkaline phosphatase at 547 IU/L & elevation in AST & ALT to 120 U/L & 144 U/L, respectively. Imaging with CT followed by MRI abdomen showed focal enlargement of the pancreatic head with dilatation of the common bile duct & the main pancreatic duct along with innumerable rim-enhancing lesions within the liver consistent with metastasis. CT Chest was also done that showed a large right suprahilar mass with mass effect on the right main bronchus. CT guided biopsy of liver lesion was performed which confirmed small cell carcinoma on pathology. Worsening jaundice prompted ERCP with EUS which showed a large mass at the major papilla site. Pancreatic duct was cannulated & sphincterotomy was performed; However, biliary cannulation could not be completed due to the size of the mass & prior history of chronic pancreatitis cannulation. Patient subsequently underwent IR guided PTC drain placement with appropriate decrease in bilirubin. Chemotherapy was initiated with carboplatin/ etoposide for metastatic small cell cancer with spread to the pancreas & liver.
Discussion: SCLC metastasis to pancreas is rare & majority of patients with pancreatic metastasis are asymptomatic upon incidental diagnosis by abdominal CT. Pancreatitis & obstructive jaundice are seldom found on initial presentation, as seen in our patient. Jaundice can result from biliary ductal obstruction if SCLC spreads to lymph nodes in the porta hepatis or the pancreatic head. Endoscopic ultrasound (EUS) is more sensitive than CT or MRI in the diagnosis of pancreatic malignancy. Metastasis to pancreas typically indicates advanced disease & clinicians should consider palliative treatment with surgical biliary bypass & chemotherapy in select patient groups which has shown to lead to clinically significant increased mean survival time.
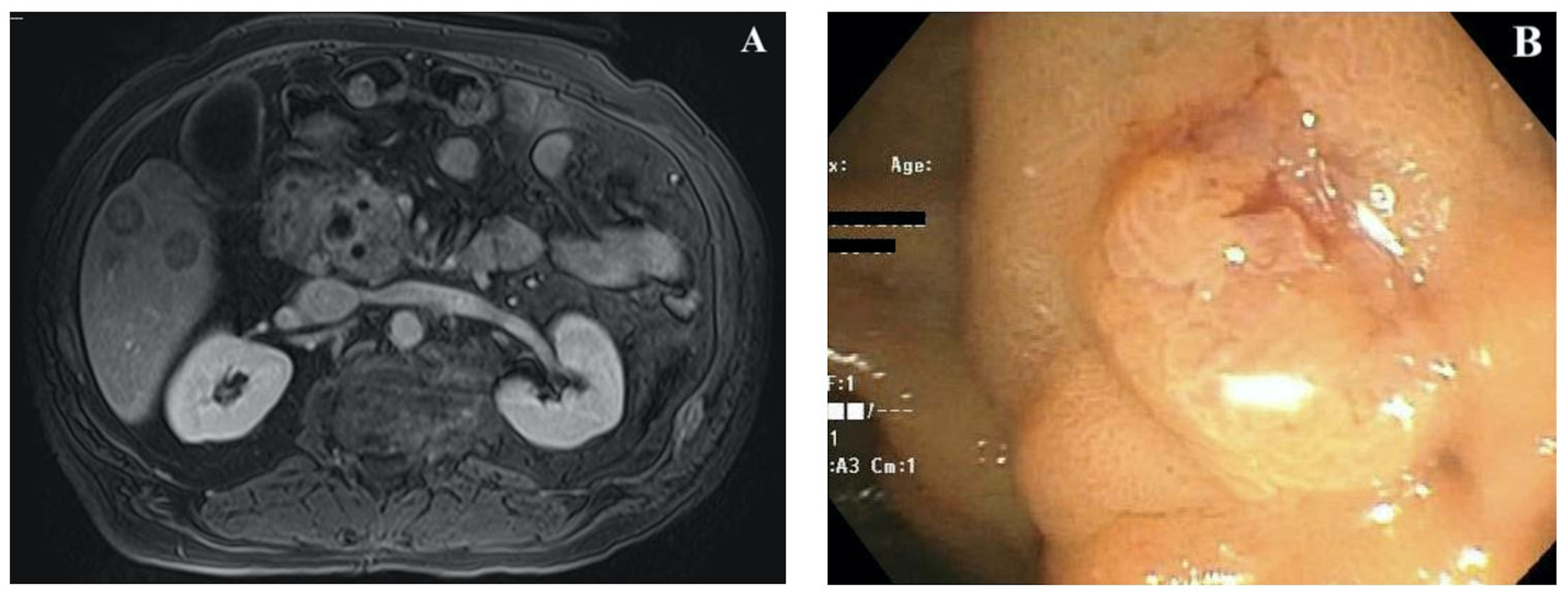
Figure: Figure 1: MRI Abdomen with contrast transverse image showing rim-enhancing lesions within the liver and focal enlargement of the pancreatic head with dilatation of the common bile duct and the main pancreatic duct (A). Endoscopic imaging showing a large fungating mass was found at the major papilla (B).
Disclosures:
Tushar Khanna indicated no relevant financial relationships.
Suhind Kodali indicated no relevant financial relationships.
Christopher Hakim indicated no relevant financial relationships.
Stefan Odabasic indicated no relevant financial relationships.
Fadi Alali indicated no relevant financial relationships.
Serge Sorser indicated no relevant financial relationships.
Jay Levinson indicated no relevant financial relationships.
Tushar Khanna, MD1, Suhind Kodali, MD2, Christopher Hakim, MD3, Stefan Odabasic, MD1, Fadi Alali, MD3, Serge Sorser, MD3, Jay Levinson, MD3. A0055 - A Rare Case of Small Cell Lung Cancer With Pancreatic Metastasis Presenting as Obstructive Jaundice, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.