Murad H. Ali, MD1, Rabia De Latour, MD2 1University at Buffalo, Buffalo, NY; 2NYU Grossman School of Medicine, Bellevue Hospital Center, New York, NY
Introduction: Gastric laparoscopic adjustable banding (LAGB) is a weight loss procedure in which a band is inflated around the proximal stomach to effectively create a pouch, satiety and resultant weight loss. A known complication of LAGB is band erosion into the lumen of the stomach, typically requiring surgical excision. We present a case report of an endoscopic removal of the eroded gastric lap band with upper endoscopy (EGD) utilizing readily available tools from the endoscopy unit.
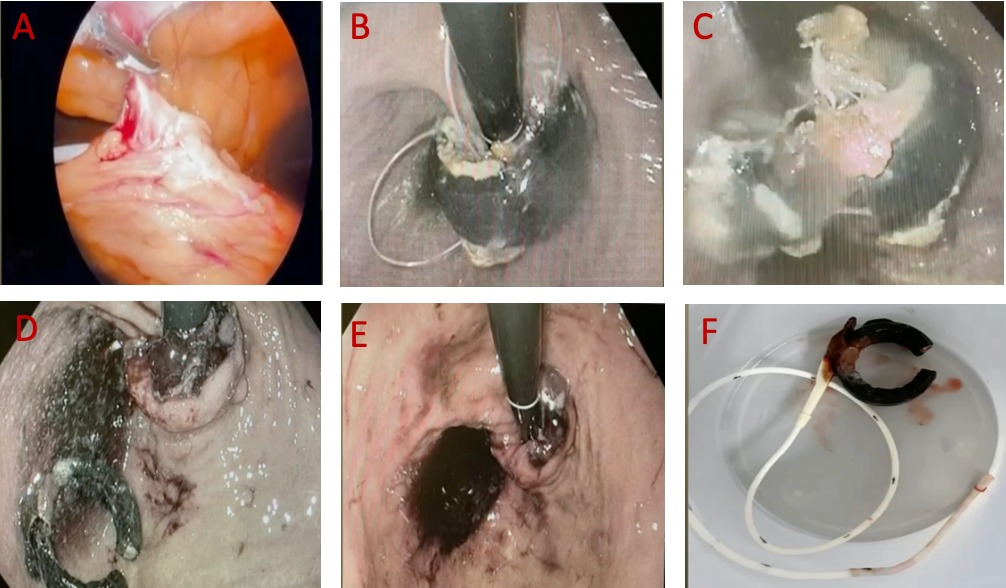
Case Description/Methods: A 45-year-old female with a history of obesity status post LAGB placement 8-years ago presents with worsening epigastric and port site pain, prompting an EGD that revealed erosion of the gastric lap band through the gastric mucosa into the lumen of the proximal stomach. Multidisciplinary plan with bariatric surgery was made for endoscopic removal of the eroded gastric lap band. Initial laparoscopy transected distal band tubing and was withdrawn orally (A). Subsequent EGD discovered eroded gastric lap band in the gastric cardia. Forceps loosened the band so that wire could loop around it, allowing lithotripter to cut the band (B,C). Lap band was pulled into the gastric lumen, using cut plastic cord left from laparoscopy in the peritoneum. Using forceps, the gastric lap band and attached cord were removed from the stomach trans-orally (D). At the end of the case, the surgical team entered the peritoneum laparoscopically and performed an air leak test on the stomach/cardia, which was negative (E). Band was successfully removed without complications (F).
Discussion: LAGB is a restrictive weight loss procedure approved by the FDA in 2001 for morbid obesity, in which a silicone band is placed around the proximal stomach and inflated with saline through a subcutaneous access port to create satiety and resultant weight loss. Despite decreased popularity, it still accounts for up to 3% of all annual weight loss surgical interventions. Band erosion is a late complication of LAGB, seen in 0.5-10% of patients. Risk factors for it include overfilling of the band with saline which can result in inflammation or ischemia, inflammatory foreign body reaction of the stomach, gastric wall injury during placement. Band erosion typically presents with non-specific abdominal pain, weight regain, discoloration of the fluid in the band. If infected it can present with sequelae of infection including port infection, sepsis and peritonitis. Our case obviated the need for invasive surgical removal or a specialized band cutter.
Figure: (A) Initial laparoscopy did not show the lap band by view as it was surrounded and encased an inflammatory rind, but band tubing was seen emerging and distal tubing was transected close to the abdominal wall. (B) A Tracer Metro long wire was advanced through the gastroscope into the stomach and looped around the band itself. (C) Soehendra lithotripter was used to cut the lap band while the gastroscope was situated within the stomach (retroflexed) visualizing the cutting of the band. (D) Using rat tooth forceps, the gastric lap band and attached cord were removed from the stomach successfully and removed trans-orally. (E) At the end of the case, the surgical team entered the peritoneum laparoscopically and performed an air leak test on the stomach/cardia, which was negative. (F) Removed gastric band ex-vivo.
Disclosures:
Murad Ali indicated no relevant financial relationships.
Rabia De Latour: Ambu – Consultant. Boston Scientific – Education/Lecturer.
Murad H. Ali, MD1, Rabia De Latour, MD2. B0473 - Endoscopic Removal of Eroded Gastric Laparoscopic Band, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.


.jpg "Murad H. Ali, MD photo")