Marshall University Joan C. Edwards School of Medicine Huntington, West Virginia
Mujtaba Mohamed, MD1, Ali Wakil, MD2 1Marshall University Joan C. Edwards School of Medicine, Huntington, WV; 2Rutgers New Jersey Medical School, Newark, NJ
Introduction: Portal vein thrombosis (PVT) is a clot formation in one of the branches of the portal vein. It is a well-known complication in patients with cirrhosis or post-abdominal surgery. Data on PVT post laparoscopic bariatric surgeries are scarce. Here we present a case of PVT post laparoscopic sleeve gastrectomy.
Case Description/Methods: A 43- years-old female with a known past medical history of hypertension, Asthma, and obesity underwent a robotic-assisted laparoscopic sleeve gastrectomy. She presented to the Emergency Department (ED) complaining of Abdominal pain 2 days after the sleeve gastrectomy operation. The patient reported doing well postoperatively till 2 days when she developed sudden epigastric abdominal pain and generalized abdominal discomfort, associated with nausea and anorexia. On arrival at the ED, her vital signs were stable and liver enzymes were normal. She had RUQ tenderness on the physical exam without guarding or rebound. The patient then had a Computed tomography (CT) of the abdomen and pelvis with IV contrast which showed occlusive left portal vein thrombosis extending to branches. She was started on oral direct Anticoagulant (DOAC) with Rivaroxaban. She had complete hypercoagulable work up with hematology which was unremarkable.
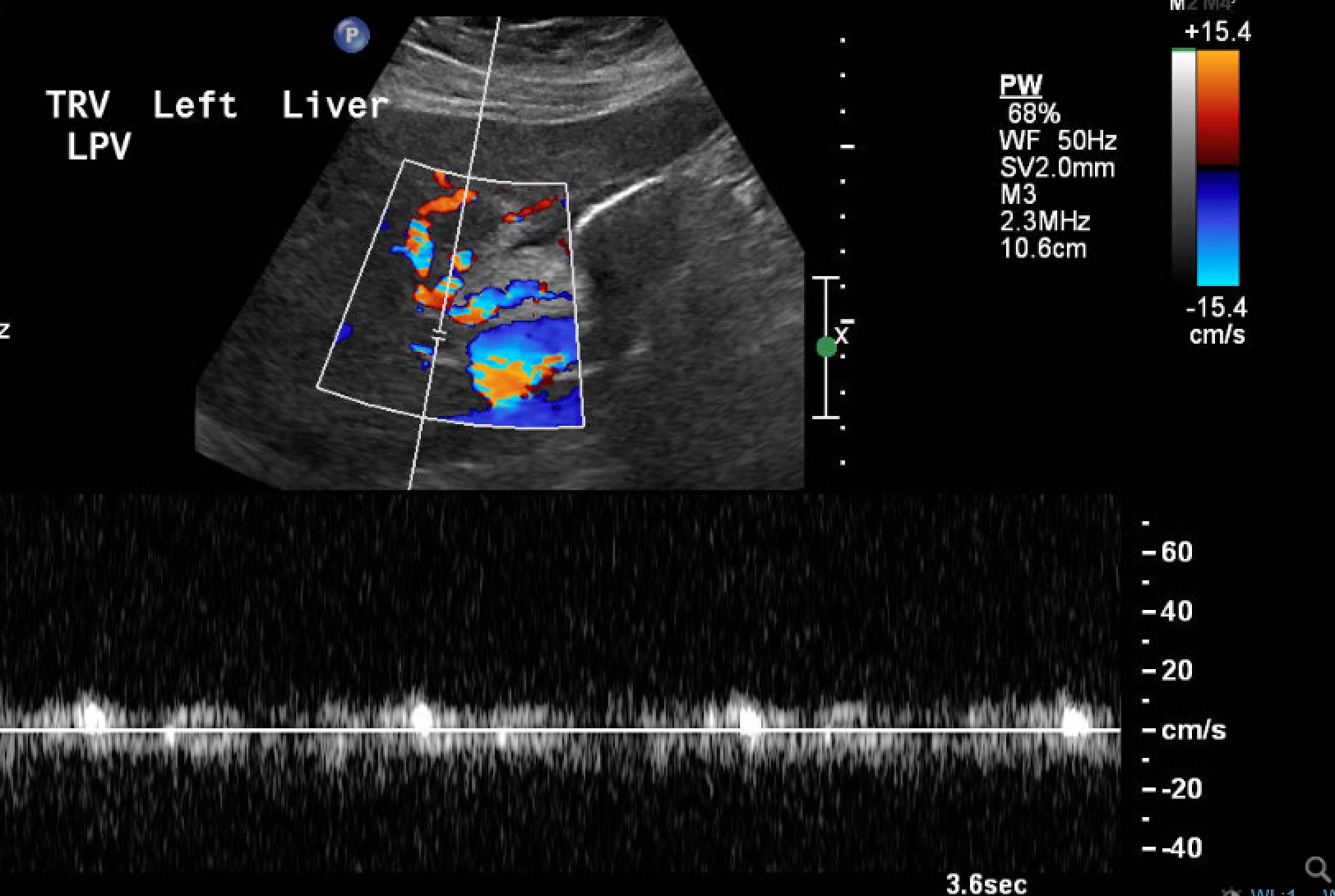
Discussion: PVT is a well-described complication of cirrhosis. in non-cirrhotic patients, the etiology of PVT can be due to systemic or local factors. A hypercoagulable state such as Factor V Leiden, antithrombin III deficiency, protein C and S deficiency, or Methylenetetrahydrofolate reductase (MTHFR) mutation is associated with higher thrombosis risk. Local factors include direct manipulation of portosystemic vessels such as during splenectomy with resultant endothelial damage and increase vascular thrombogenicity. A gastric sleeve is less likely to cause PVT since it only involves the short gastric vein. However, with the use of laparoscopic surgical techniques, there has been an increase in reported PVT. It is suspected that an increase in intra-abdominal pressure during carbon dioxide insufflation causes a pro-thrombotic state by decreasing venous and portal blood flow. The diagnosis of PVT post-operatively requires a high level of suspicion and can be made with abdominal imaging such as Ultrasound with color doppler or CT with IV contrast. The treatment is usually anticoagulation with the goal of recanalization of the portal vein on repeat imaging to prevent the development of non-cirrhotic portal hypertension in these patients.
Figure: Color doppler showing left portal vein thrombosis
Disclosures:
Mujtaba Mohamed indicated no relevant financial relationships.
Ali Wakil indicated no relevant financial relationships.
Mujtaba Mohamed, MD1, Ali Wakil, MD2. E0566 - Portal Vein Thrombosis Post Laparoscopic Sleeve Gastrectomy, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.