University of Missouri-Kansas City Kansas City, MO
Ifrah Fatima, MD1, Mariam Haji, MD2, Wael T. Mohamed, MD2, Valerica Mateescu, MD2, Sheshadri Madhusudhana, MD2, Anuj Shrestha, MD2 1University of Missouri-Kansas City, Kansas City, MO; 2University of Missouri, Kansas City, MO
Introduction: Vanishing bile duct syndrome (VBDS) is an uncommon, acquired form of cholestatic liver disease characterized by hepatic ductopenia and cholestasis. We present a case of VBDS as the initial manifestation of classical Hodgkin lymphoma (CHL), with normalization of liver enzymes after treatment with standard-dose chemotherapy- Doxorubicin, Bleomycin, Vinblastine, and Dacarbazine (ABVD).
Case Description/Methods: A 26-year-old female presented with nausea, weight loss, right-sided neck mass, pruritus, and yellowing of eyes and skin. She was on Celecoxib and Prednisone 40mg (5 days), for back pain associated with scoliosis. On physical exam, she had jaundice and cervical lymphadenopathy. Labs were significant for a total bilirubin of 22 mg/dL and elevated aspartate transaminase (AST) 91 U/L, alanine transaminase (ALT) 108 U/L, alkaline phosphatase 662 U/L, INR 1.3. Ultrasound abdomen showed mild hepatosplenomegaly but no bile duct dilatation. Hepatitis panel, EBV, and HIV were negative. CA 19-9 and AFP were normal. MRCP ruled out obstructive process/mass. Liver biopsy revealed prominent cholestasis and Kupffer cell hyperplasia with focal perivenular hepatocyte dropout and loss of bile ducts, greater than 50%- consistent with idiopathic cholestasis with ductopenia, also known as VBDS. PET/CT of neck showed extensive supra-diaphragmatic lymphadenopathy, large nodal mass in the neck, and superior mediastinum with associated mass effect. Biopsy of right cervical lymph node showed CHL, nodular sclerosis type. Immunohistochemical staining was positive for CD30, CD15, and PAX5 (weak) supporting the diagnosis. She was started on Gemcitabine, Cyclophosphamide, and Dexamethasone as liver-sparing agents. However, liver enzymes remained elevated. She was started on standard chemotherapy for CHL – ABVD along with Rituximab (ABVD-R) with dose-adjusted vinblastine for cycles 1-2. She then completed cycles 3 to 6 of ABVD. Post C4, PET/CT showed a complete metabolic response. Liver enzymes normalized progressively with chemotherapy
Discussion: Idiopathic cholestasis with ductopenia can be seen as a paraneoplastic phenomenon in CHL even in the absence of direct hepatic involvement by lymphoma. The primary goal of treatment for hepatic injury was treatment of CHL as able with her liver dysfunction. Our case illustrates the use of standard ABVD even with elevated LFTs in the setting of CHL and VBDS. Repeat liver biopsy was not done as the patient remains in complete remission at oncology follow up.
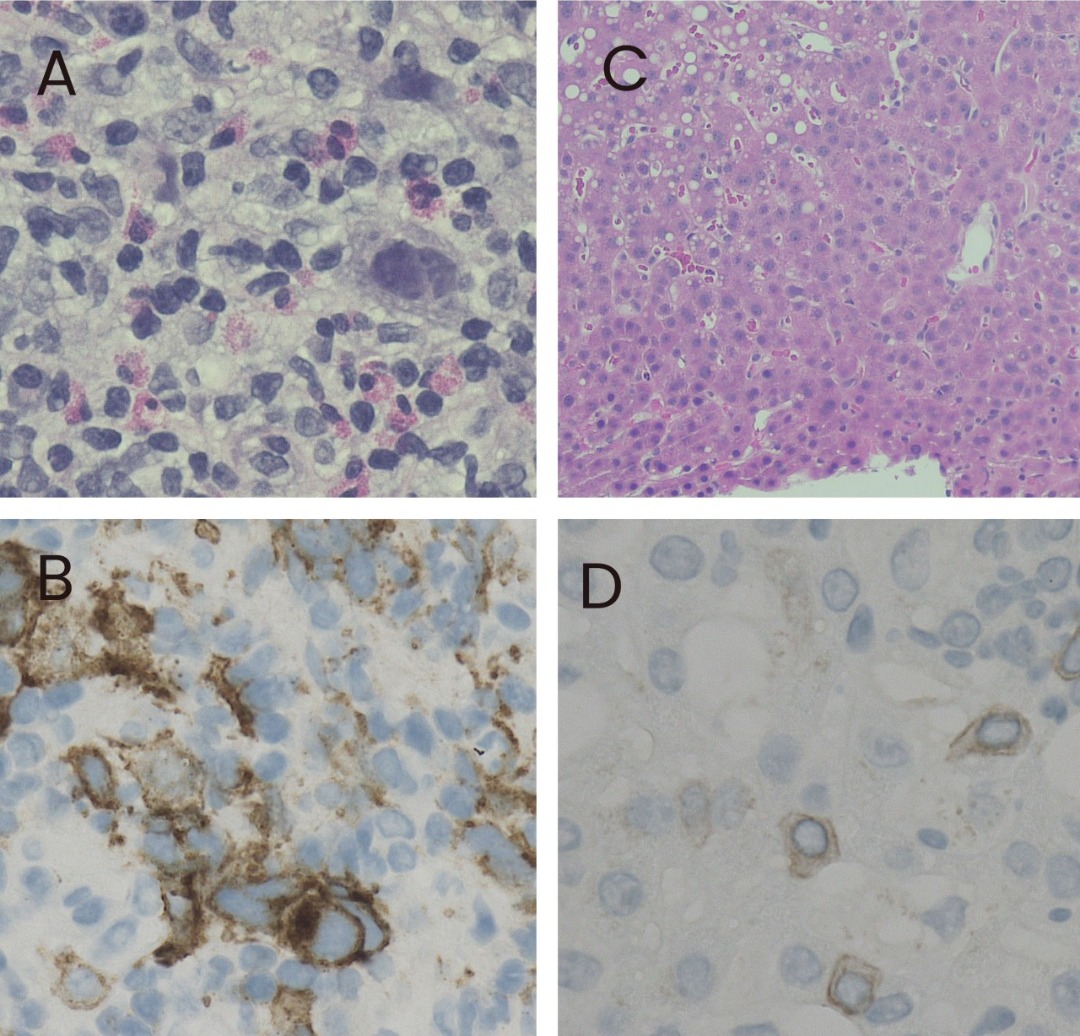
Figure: A: Lymph node biopsy, Hematoxylin & Eosin (H&E) stain, 200X B: Lymph node biopsy, CD30 immunohistochemical (IHC) stain, 100X (highlights CD30+ Reed-Sternberg and Hodgkin cells) C: Liver biopsy, H&E stain, 100X (shows bile duct loss) D: Liver biopsy, CK7 IHC, 200X (shows vanishing bile ducts, only isolated cells CK7+ with no intact bile ducts)
Disclosures:
Ifrah Fatima indicated no relevant financial relationships.
Mariam Haji indicated no relevant financial relationships.
Wael Mohamed indicated no relevant financial relationships.
Valerica Mateescu indicated no relevant financial relationships.
Sheshadri Madhusudhana indicated no relevant financial relationships.
Anuj Shrestha indicated no relevant financial relationships.
Ifrah Fatima, MD1, Mariam Haji, MD2, Wael T. Mohamed, MD2, Valerica Mateescu, MD2, Sheshadri Madhusudhana, MD2, Anuj Shrestha, MD2. E0582 - Vanishing Bile Duct Syndrome as a Presentation of Classical Hodgkin’s Lymphoma, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.