University of Connecticut Health Center Farmington, CT
Sriya Bhumi, MD, MBA1, Jaimy Villavicencio Kim, MD2, Elizabeth Richardson, DO3 1University of Connecticut Health Center, Farmington, CT; 2UConn Health, Farmington, CT; 3Hartford Healthcare, Hartford, CT
Introduction: Gastric cancer usually has a grim prognosis given that it is often diagnosed at advanced stages. Predisposed patients with gastric intestinal metaplasia have an increased risk of progression to gastric cancer by 3 fold. For organ transplant recipients, there is a 4 time increased risk of cancer, with higher levels of immunosuppression being linked to a more aggressive course. Literature is sparse when it comes to surveillance of gastric cancer in transplant patients, regardless of presence of intestinal metaplasia. We propose a case that reveals how aggressively gastric cancer could progress when a predisposed patient is also immunosuppressed.
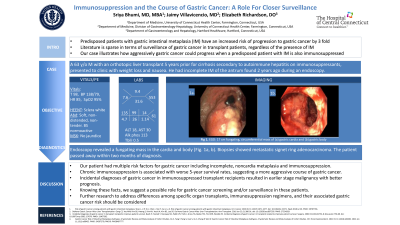
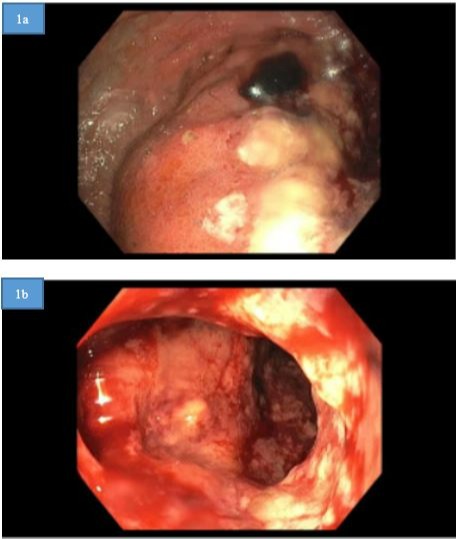
Case Description/Methods: A 63 year old male with intestinal metaplasia and an orthotopic liver transplant 5 years prior for cirrhosis secondary to autoimmune hepatitis on immunosuppressants, presented to clinic with weight loss and nausea. The remaining review of systems was negative. He had been diagnosed with incomplete intestinal metaplasia of the antrum 2 years ago. His vitals were stable and abdominal exam was benign. Laboratory tests were significant for microcytic anemia. Esophagogastroduodenoscopy revealed a fungating mass in the cardia and body, of which biopsies showed metastatic signet ring adenocarcinoma (Fig. 1a,b). The patient had multiple re-hospitalizations for malignant ascites and failure to thrive. The patient passed away within two months of diagnosis.
Discussion: Our patient had numerous risk factors that predisposed him to developing gastric cancer, including incomplete, noncardia metaplasia, and immunosuppression. The chronicity of immunosuppression is associated with worse 5-year survival rates, suggesting how the course of the cancer is likely to be more rapidly progressive with the addition of immunosuppression. Incidental diagnoses of gastric cancer, even in immunosuppressed transplant recipients, resulted in an earlier stage malignancy with better prognosis. Further research should be conducted to address differences among specific organ transplants, immunosuppression regimens and their associated gastric cancer course. While intestinal metaplasia and immunosuppression are independent risk factors for developing gastric cancer, our case suggests how immunosuppression contributes to the aggressive course of gastric cancer and calls for closer surveillance in this population.
Figure: Figure 1. 17 cm fungating, circumferential mass of (a) gastric cardia and (b) gastric body
Disclosures:
Sriya Bhumi indicated no relevant financial relationships.
Jaimy Villavicencio Kim indicated no relevant financial relationships.
Elizabeth Richardson indicated no relevant financial relationships.
Sriya Bhumi, MD, MBA1, Jaimy Villavicencio Kim, MD2, Elizabeth Richardson, DO3. D0719 - Immunosuppression and the Course of Gastric Cancer: A Role for Closer Surveillance, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.