Rahul R. Thakkar, MD1, Erik Rahimi, MD2 1Baylor Scott & White Round Rock, Round Rock, TX; 2Baylor Scott and White Round Rock/Lakeway, Round Rock, TX
Introduction: Pleural effusions due to pancreaticopleural fistulas (PPFs) are exceptionally rare, often presenting as recurrent, left-sided effusions in middle-aged men with a chronic history of alcohol use and pancreatitis.1-3 Rarely, PPFs may occur in elderly patients and present as bilateral pleural effusions, as illustrated in this case.
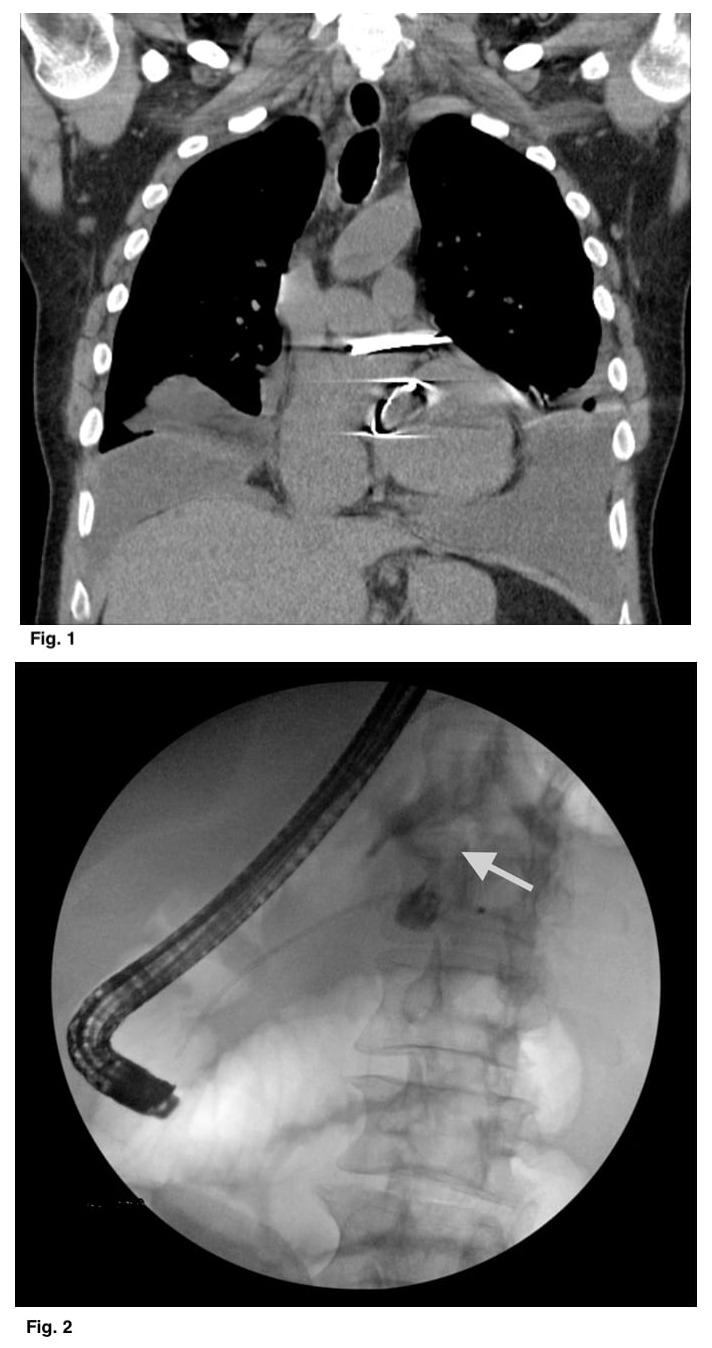
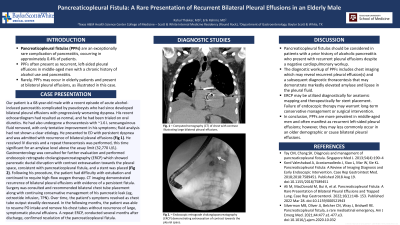
Case Description/Methods: Our patient is a 68-year-old male with a recent episode of acute alcoholic pancreatitis who had since developed bilateral pleural effusions with progressively worsening dyspnea. His recent echocardiogram had resulted as normal and he had been started on oral diuretics. He had also undergone a thoracentesis with ~1.6 L serosanguinous fluid removed, with only tentative improvement in his symptoms; fluid analysis had not shown a clear etiology. He presented to ED with persistent dyspnea and was admitted with recurrence of bilateral pleural effusions (Fig 1). He received IV diuresis and a repeat thoracentesis was performed, significant for an amylase level above the assay limit (32,770 U/L). Gastroenterology was consulted for further evaluation and performed endoscopic retrograde cholangiopancreatography (ERCP) which showed pancreatic ductal disruption with contrast extravasation towards the pleural space – consistent with pancreaticopleural fistula – warranting stent placement (Fig 2). Following his procedure, the patient had difficulty with extubation and continued to require high-flow oxygen therapy. CT imaging demonstrated recurrence of bilateral pleural effusions with evidence of a persistent fistula. Surgery was consulted and recommended bilateral chest tube placement along with continuing conservative management of his pancreatic leak (eg, octreotide infusion, TPN). Over time, the patient’s symptoms resolved as chest tube output steadily decreased. In the following months, the patient was able to resume PO intake and remove his chest tubes without recurrence of large, symptomatic pleural effusions. A repeat ERCP, conducted several months after discharge, confirmed resolution of the pancreaticopleural fistula.
Discussion: Pancreaticopleural fistulas should be considered in patients with a prior history of alcoholic pancreatitis who present with recurrent pleural effusions, which may rarely occur bilaterally. Although typically occurring in middle-aged male patients, PPFs may less commonly present in the elderly. Lastly, failure of endoscopic therapy may warrant prolonged conservative management or surgical intervention.
Figure: Fig. 1: CT chest with contrast illustrating bilateral pleural effusions Fig. 2: ERCP demonstrating extravasation of contrast towards pleural space
Disclosures:
Rahul Thakkar indicated no relevant financial relationships.
Erik Rahimi indicated no relevant financial relationships.
Rahul R. Thakkar, MD1, Erik Rahimi, MD2. A0071 - Pancreaticopleural Fistula: A Rare Presentation of Recurrent Bilateral Effusions in an Elderly Male, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.

.jpg "Rahul R. Thakkar, MD photo")