Asad Rehman, DO1, Toshio Nagamoto, MD2, Erica Tirado, DO2 1HCA West Florida Largo Medical Center, Largo, FL; 2Good Samaritan Regional Medical Center, Corvallis, OR
Introduction: Sclerosing mesenteritis, also called mesenteric panniculitis, describes a rare fibroinflammatory disorder. Acute or insidious in onset, it predominates in males over 60. Small intestine involvement is most common and can present as idiopathic, autoimmune or malignant. We report an unusual case of a previously healthy young male with mesenteritis related to follicular lymphoma.
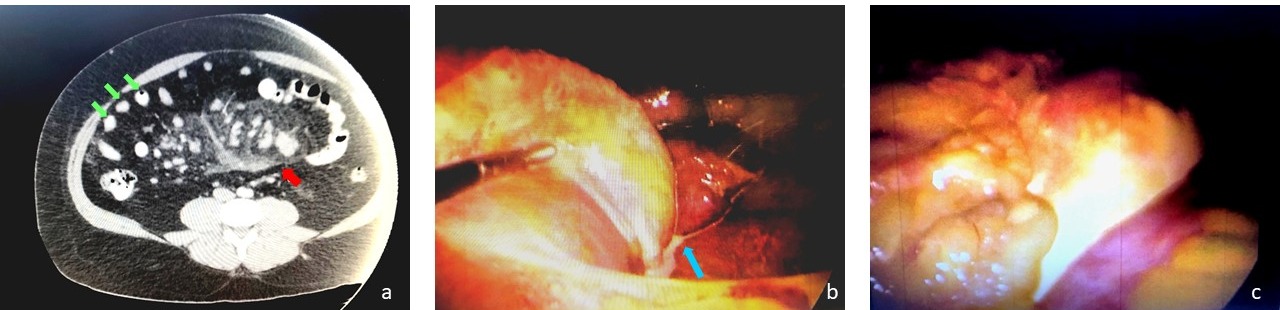
Case Description/Methods: A 30-year-old male with a past medical history of obesity (BMI 45) and hyperlipidemia presented with mild diffuse abdominal pain and slightly elevated liver enzymes (AST 58, ALT 118). Family history included a grandfather with lymphoma in his 50s. CT Abdomen showed enlarged mesenteric lymph nodes measuring between 2.2-2.7 cm and coalescent, rim-enhancing cystic lesions with low-attenuation in the root of the small bowel mesentery (a). An area of fat around the mesenteric vessels and a fibrous band separating inflamed fat from mesentery was also seen, called fat ring sign and pseudocapsule, respectively. Laparoscopy was performed and the band was taken down with bipolar energy. Distorted omentum, small bowel edema, prominent lymph channels and chylous ascites were noted (b,c). Lymph node biopsy showed 50% of monoclonal B-cells expressing CD19, CD20 bright, CD10, and dim kappa light chain on flow cytometry, indicating follicular B-cell lymphoma.
Discussion: Mesenteritis presents with nonspecific symptoms and is usually diagnosed in older adults with histories of abdominal surgeries. Along with histopathology, cytometry, and CT, PET can further diagnose this condition, as increased contrast uptake suggests co-existing mesenteric deposits, particularly in patients with lymphoma. Although mild cases have shown to resolve spontaneously, glucocorticoids and tamoxifen are first line therapy, while colchicine, azathioprine or cyclophosphamide are used adjunctly. Tamoxifen can be continued indefinitely to downregulate fibrosis, as the rate of recurrence and complications, including obstruction and perforation, is clinically significant. Follow up with patients is imperative as co-existing malignancies develop in up to 70% of patients with mesenteritis and include lymphomas, urogenital, and gastrointestinal carcinomas. Although literature is limited, mesenteritis should be included in the differential for nonspecific GI symptoms, regardless of advanced age. As in our case, this can treat potential malignancies early and avoid morbid complications, especially in a setting of familial history of cancer.
Figure: Image a: Enlarged mesenteric lymph nodes (green arrows) noted on initial CT with fat ring sign (red arrow). b: Prominent lymph channels with chylous ascites leading up to nodes were noted on laparoscopy (blue arrow). c: Distorted omentum with associated small bowel edema.
Disclosures:
Asad Rehman indicated no relevant financial relationships.
Toshio Nagamoto indicated no relevant financial relationships.
Erica Tirado indicated no relevant financial relationships.
Asad Rehman, DO1, Toshio Nagamoto, MD2, Erica Tirado, DO2. E0652 - Sclerosing Mesenteritis in the Setting of Follicular Lymphoma in a Young Male, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.

.jpg "Asad Rehman, DO photo")