University of California San Francisco San Francisco, CA
Nathan Alhalel, MD, MPH1, Ralph Alhalel, MD2 1University of California San Francisco, San Francisco, CA; 2Rio Grande Gastroenterology Consultants, Mission, TX
Introduction: Follicular lymphoma (FL) accounts for approximately 4% of gastrointestinal (GI) lymphomas (1). Of the follicular lymphomas found in the GI tract, duodenal-type follicular lymphoma (D-FL) make up 38-81% of cases (2-4). D-FL is often incidentally discovered, lack invasion into deeper layers of the GI tract, and are indolent in nature (5). The clinical stage at time of diagnosis often predicts probability of disease progression (6). Given the excellent prognosis and rare occurrence of progression to high stage FL or transformation to diffuse large B cell lymphoma, a “wait and see” therapeutic approach is often taken (4,7). We report a case of D-FL here.
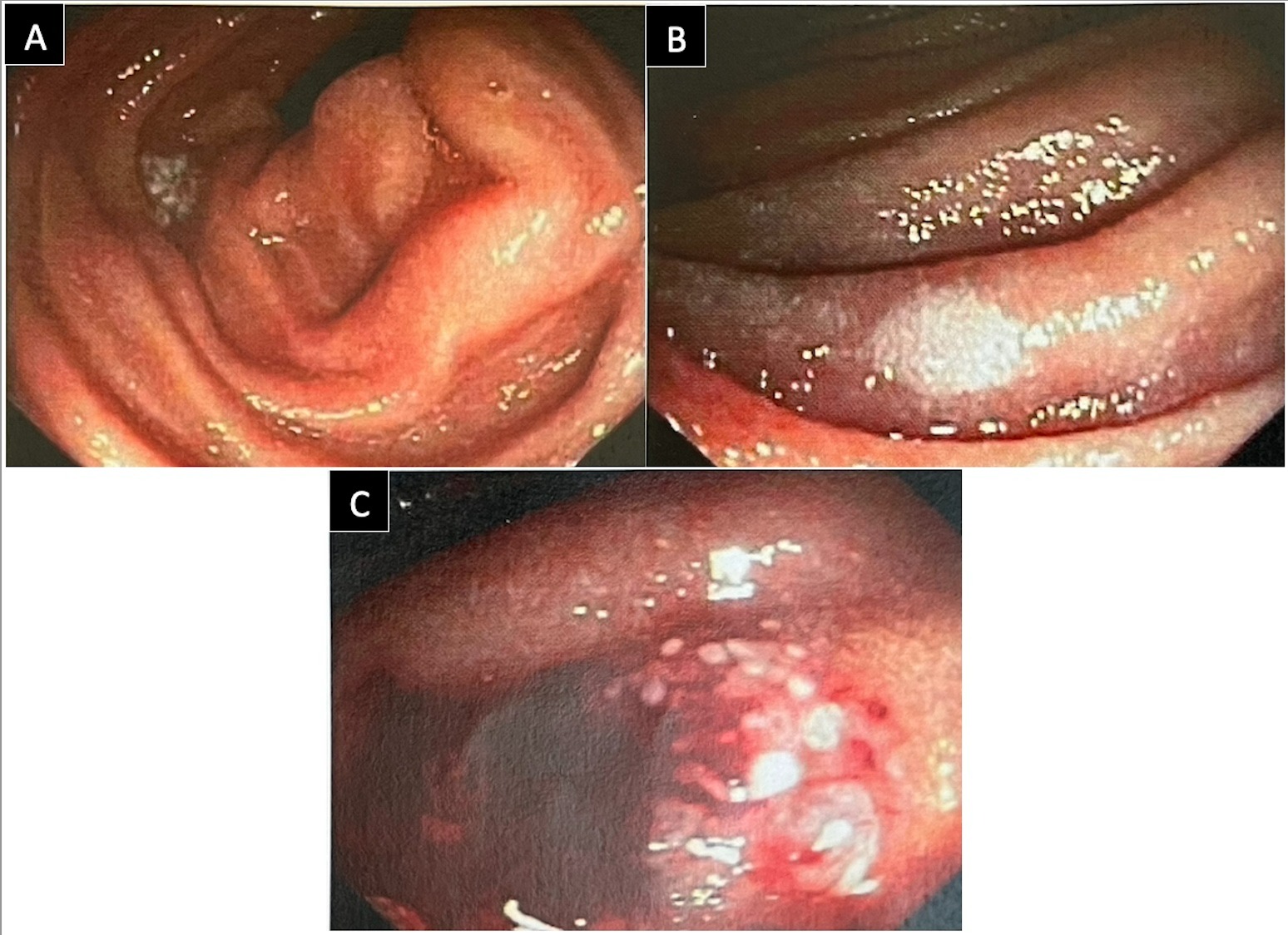
Case Description/Methods: A 39-year-old female with no pertinent past medical history presented with refractory acid reflux. Her endoscopy was notable for gastritis, duodenal atrophy, and three 5-mm pale nodules in the second part of the duodenum (Figure 1A-1C). Initial biopsy of these polyps showed atypical lymphoid follicular aggregates. Outside pathologists’ subsequent review noted atypical lymphoid cells positive for CD10, BCL-2, BCL-5, and CD20 markers, consistent with duodenal follicular lymphoma. Further workup with small bowel enteroscopy to the mid-jejunum and colonoscopy were normal. LDH, SPEP with immunofixation, HIV, hepatitis serologies, and full body CT were unremarkable. The patient was diagnosed with stage I D-FL per the Lugano staging system for gastrointestinal lymphomas, and a “wait and wait” approach was recommended by oncology.
Discussion: D-FL typically presents with multiple low-stage, white nodules in the second portion of the duodenum, as in our case. Because lesions are rarely solitary in 78-85% D-FL cases, thorough small bowel assessment with enteroscopy or capsule endoscopy is warranted (3,4). Radiation has been shown to be effective in limited disease and is the most common form of treatment (8-10). Chemotherapy, Rituximab, and surgery can also used as monotherapy or in combination therapy (4). However, the “watch and wait” approach has been found to be equally effective and is the most common approach amongst oncologists in the United States (11).
Figure: Figure 1: Endoscopic images of the duodenal second portion. Three distinct 5-mm pale nodules were seen and biopsies. First, second, and third lesions are seen in figure 1A, 1B, and 1C, respectively.
Disclosures:
Nathan Alhalel indicated no relevant financial relationships.
Ralph Alhalel indicated no relevant financial relationships.
Nathan Alhalel, MD, MPH1, Ralph Alhalel, MD2. E0666 - Multifocal Duodenal-type Follicular Lymphoma Found Incidentally on Diagnostic Endoscopy, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.