Baton Rouge General Medical Center Baton Rouge, LA
Ashley Capace, MD, Jeremy Polman, DO, MS, MBA, Karthik Reddy, MD Baton Rouge General Medical Center, Baton Rouge, LA
Introduction: Mycotic aortitis is an uncommon diagnosis that is almost universally fatal if not diagnosed and treated quickly. Primary aortoenteral fistula is a rare, equally life-threatening complication of mycotic aortitis due to localized inflammation of the aorta and the anatomical proximity of the bowel. The duodenum is the most common segment of bowel involved as it is located directly anterior to the aorta. Just over 250 cases have been documented between 1951 and 2010. With mortality approaching 100%, a high clinical suspicion is required for timely diagnosis and treatment.
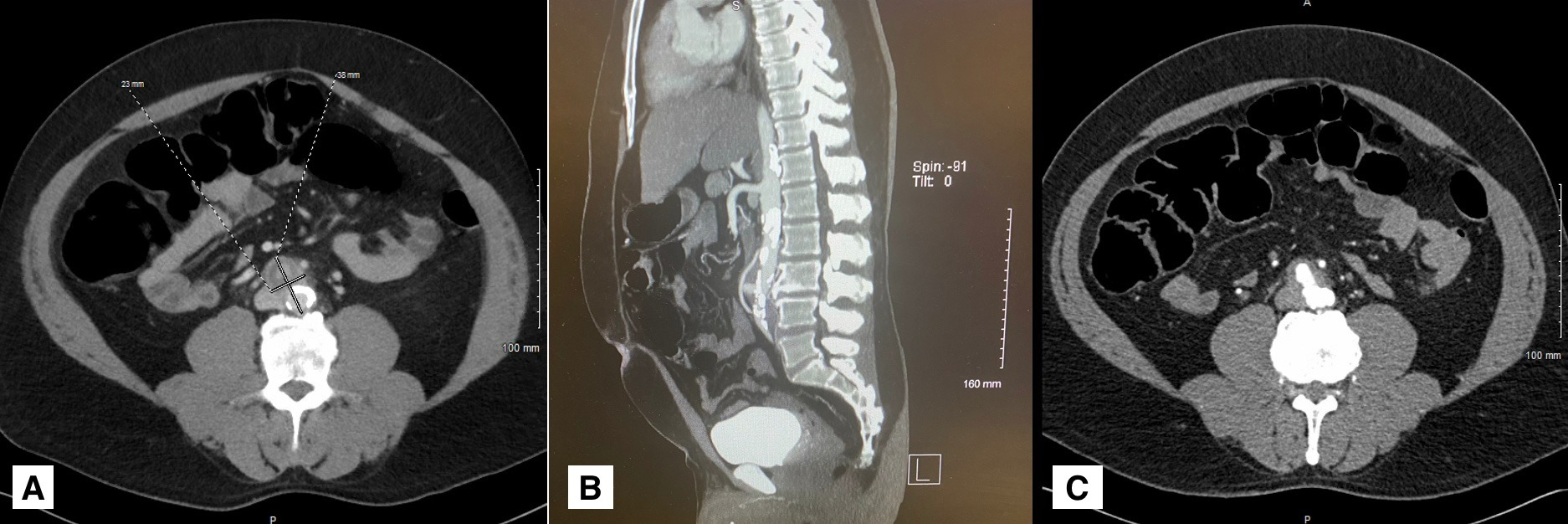
Case Description/Methods: Here we present the case of a 54-year-old male with a 3 month history of vague abdominal pain. He was recently diagnosed with an unspecified abdominal mass, suspected to be malignancy. A PET scan revealed a hypermetabolic retroperitoneal mass with a biopsy planned at a later date. Before biopsy, the patient had acutely worsening abdominal pain and presented to the emergency department. An abdominal angiogram revealed an irregular saccular infrarenal abdominal aortic aneurysm with a mural thrombus and periaortic fat stranding with mural enhancement consistent with aortitis [A, B, C]. These findings were in the same location as the previously noted hypermetabolic retroperitoneal mass. Evaluation also revealed Methicillin sensitive Staphylococcus aureus bacteremia. The patient was diagnosed with mycotic aortitis and initiated on Ertapenem. He subsequently underwent an open procedure for aortic aneurysm repair with extensive debridement, where he was found to have a primary aortoduodenal fistula (PADF) with extensive spillage of duodenal contents. The area was debrided and the fistula repaired with plans to repair the aneurysm at a later time following resolution of severe localized inflammation.
Discussion: PDAF is a difficult diagnosis to make due to its low incidence and often vague symptoms. The classic triad of symptoms, in order of most to least common, includes gastrointestinal bleed, abdominal pain, and a pulsatile abdominal mass. However, this triad is only present in 10-11% of cases. Although gastrointestinal bleeding is the most common symptom, it is not present in over 60% of patients. Even with proper treatment, aortitis and primary aortoenteral fistulas both have an exceedingly high mortality rate. Quickly recognizing mycotic aortitis and planning an open surgical intervention led to the diagnosis of PADF in our patient which may have prevented his mortality.
Figure: A) Transverse slice from CT abdomen and pelvis revealing 23mm x 38mm abdominal aortic aneurysm. B) Sagittal slice from CT Abdomen and pelvis with IV contrast revealing abdominal aortic aneurysm with thrombus. C) Transverse slice from CT abdomen and pelvis with IV contrast revealing extravasation of blood from the abdominal aorta into the duodenum and surrounding tissues.
Disclosures:
Ashley Capace indicated no relevant financial relationships.
Jeremy Polman indicated no relevant financial relationships.
Karthik Reddy indicated no relevant financial relationships.
Ashley Capace, MD, Jeremy Polman, DO, MS, MBA, Karthik Reddy, MD. E0669 - Primary Aortoduodenal Fistula as a Complication of Mycotic Aortitis, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.