Staten Island University Hospital Staten Island, New York
Jarin Prasa, DO1, Syed S. Karim, DO2, Muhammad Abdullah, MD2 1Staten Island University Hospital, Staten Island, NY; 2Coney Island Hospital, Brooklyn, NY
Introduction: CMV infections of the colon are common but exceedingly rare in the stomach and usually only found in immunocompromised individuals. We present a case of CMV gastritis where no certain risk factors were found for CMV in an otherwise healthy man.
Case Description/Methods: A 54 year old male with a history of H.pylori gastritis and erosions noted on an EGD around 10 years ago and asthma, presented with epigastric pain, bloating, and vomiting for 2 weeks. He was an active smoker but denied any alcohol or illicit drugs. He attributed to frequent use of his albuterol inhalers, but review of systems and his physical exam were otherwise unremarkable. Labs demonstrated mild elevations in ALT and AST, but a normal CBC with differential and BMP. CT demonstrated normal lungs, fatty liver but otherwise normal liver, spleen and pancreas, no lymphadenopathy, and thickening of the stomach. EGD revealed a granular inflamed mucosa surrounding the antrum spreading up in the incisura and distal body highly suspicious for malignancy. Pathology revealed chronic gastritis with erosions with rare enlarged epithelial glandular cells with intranuclear and cytoplasmic Inclusions consistent with CMV gastritis and negative for H.pylori. He initially improved on PPI therapy alone. Upon follow up, HIV was checked and found negative. He was then referred to an infectious disease specialist for proper antiviral treatment and dosing.
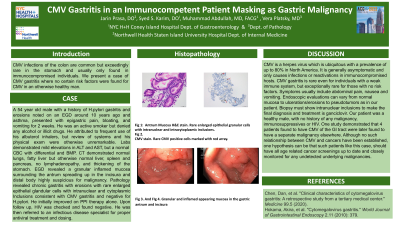
Discussion: CMV is a herpes virus which is ubiquitous with a prevalence of up to 80% in North America. It is generally asymptomatic and only causes infections or reactivations in immunocompromised hosts. CMV gastritis is rare even for individuals with a weak immune system, but exceptionally rare for those with no risk factors. Symptoms usually include abdominal pain, nausea and vomiting. Endoscopic evaluations can vary from normal mucosa to ulcerations/erosions to pseudotumors as in our patient. Biopsy must show intranuclear inclusions to make the final diagnosis and treatment is ganciclovir. Our patient was a healthy male, with no history of any malignancy, immunosuppressives or HIV. One study demonstrated that 4 patients found to have CMV of the GI tract were later found to have a separate malignancy elsewhere. Although no such relationship between CMV and cancers have been established, one hypothesis can be that such patients like this case, should have all age related cancer screenings up to date and closely monitored for any undetected underlying malignancies.
Disclosures:
Jarin Prasa indicated no relevant financial relationships.
Syed Karim indicated no relevant financial relationships.
Muhammad Abdullah indicated no relevant financial relationships.
Jarin Prasa, DO1, Syed S. Karim, DO2, Muhammad Abdullah, MD2. E0698 - CMV Gastritis in an Immunocompetent Patient Masking as Gastric Malignancy, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.