Abdul Aziz S. Siddiqui, MD, Nicholas Nassif, MD, Nadia Huq, MD Advocate Aurora Healthcare, Milwaukee, WI
Introduction: The association between acute pancreatitis and ulcerative colitis is described in literature, with a majority of pancreatitis in this population being drug-induced. Endoscopic modalities offer a pathway to diagnosis and is a mainstay in differentiating IBD and associated conditions such as autoimmune pancreatitis. In these situations procedural approach to diagnosis should always be guided by clinical gestalt.
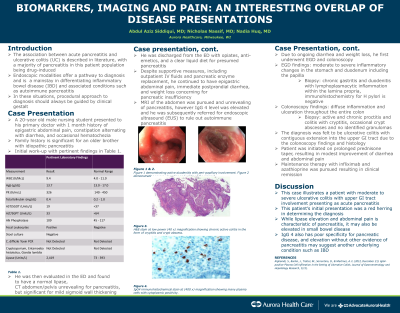
Case Description/Methods: A 20-year old male presents to his primary doctor with 1 month history of epigastric abdominal pain, constipation alternating with diarrhea, and occasional hematochezia. Family history is significant for a brother with idiopathic pancreatitis. Initial work-up was significant for an elevated lipase. He was then evaluated in the ED with a CT abdomen unrevealing for pancreatitis, but significant for mild sigmoid wall thickening. He was discharged home with opiates, anti-emetics and a clear liquid diet for presumed pancreatitis. Despite outpatient IV fluids and pancreatic enzyme replacement, he continued to have epigastric abdominal pain, immediate postprandial diarrhea, and weight loss concerning for pancreatic insufficiency. MRI abdomen was pursued and unrevealing of pancreatitis, however IgG 4 level was elevated and he was subsequently referred for EUS to rule out autoimmune pancreatitis. Due to ongoing diarrhea and weight loss, he first underwent EGD and colonoscopy which was significant for moderate inflammatory changes in the stomach and duodenum including the papilla, as well as diffuse inflammation and ulceration throughout the entire colon. Biopsies revealed chronic proctitis and colitis as well as chronic gastritis and duodenitis. The colonoscopy and histological findings suggested a diagnosis of UC with contiguous extension into the upper GI tract. Patient was initiated on prolonged prednisone taper, resulting in modest improvement of diarrhea and abdominal pain. Maintenance therapy with infliximab and azathioprine was pursued.
Discussion: This case illustrates a patient with moderate to severe ulcerative colitis with upper GI tract involvement presenting as acute pancreatitis. This patient’s acute pancreatitis acted as a red herring in determining diagnosis, and while lipase elevation and abdominal pain is characteristic of pancreatitis, it may also be elevated in small bowel disease. In addition, IgG 4 also has poor specificity for pancreatic disease and elevation without other evidence of pancreatitis may suggest another underlying condition such as IBD.
Disclosures:
Abdul Aziz Siddiqui indicated no relevant financial relationships.
Nicholas Nassif indicated no relevant financial relationships.
Nadia Huq indicated no relevant financial relationships.
Abdul Aziz S. Siddiqui, MD, Nicholas Nassif, MD, Nadia Huq, MD. E0417 - Biomarkers, Imaging and Pain: An Interesting Overlap of Disease Presentations, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.