Andreas W. Bub, MD1, Jaspreet Suri, MD2, Amr Sayed, MD3 1Stamford Hospital, Stamford, CT; 2Norwalk Hospital/Yale, Norwalk, CT; 3Norwalk Hospital, Norwalk, CT
Introduction: Sweet's syndrome (SS), a subtype of neutrophilic dermatosis (ND), is an uncommon skin disorder characterized by the abrupt appearance of painful erythematous skin lesions, fever, and neutrophilia. Diagnosis of SS is made via biopsy showing a dense neutrophilic infiltrate of the dermis and epidermal sparing. SS is associated with hematologic malignancies or drug reactions and less commonly with inflammatory bowel disease (IBD). Treatment of SS, and other NDs, mirrors treatment of the underlying condition and is typically steroid responsive. Identification is important as SS is an extra systemic manifestation of underlying disease and indicates a poor prognosis. We present an 18 year old male with SS as a manifesting symptom of IBD.
Case Description/Methods: An 18 year old male presented with 1 month of abdominal pain, oral ulcerations, hematochezia, and a left lower extremity lesion. He had a diffusely tender abdomen, multiple ulcers bilaterally on his buccal mucosa, cheilitis, and a 1 cm ulcerated lesion on his left leg. He was febrile and blood tests revealed anemia, thrombocytosis, neutrophilia, elevated inflammatory markers, and a positive C-ANCA. His leg and oral lesions were biopsied as well as a cratered esophageal ulcer found during endoscopy. Sigmoidoscopy demonstrated a circular ulceration of the anal mucosa and severe patchy inflammation in the descending and sigmoid colon. He was started on methylprednisolone for empiric treatment of presumed IBD. The skin biopsy showed ND with an interstitial and perivascular inflammatory infiltrate with epidermal necrosis without vasculitis most consistent with SS. He was diagnosed with Crohn’s Disease and has seen improvement of his skin lesions, oral lesions, and abdominal symptoms after a prolonged steroid taper.
Discussion: While NDs are well described in association with IBD, SS is not a subtype of ND that commonly occurs with less than 100 cases described. Biopsy is the definitive diagnostic study and should be done promptly as ND’s differential includes drug-reaction, malignancy, and the skin lesions may appear similar to infectious lesions. The two former conditions will respond to treatment though may relapse if not identified, and the latter will be exacerbated by immunosuppression. For Physicians treating IBD, knowledge of the appearance of ND can ensure prompt biopsy and initiation, or withdrawal, of appropriate therapies.
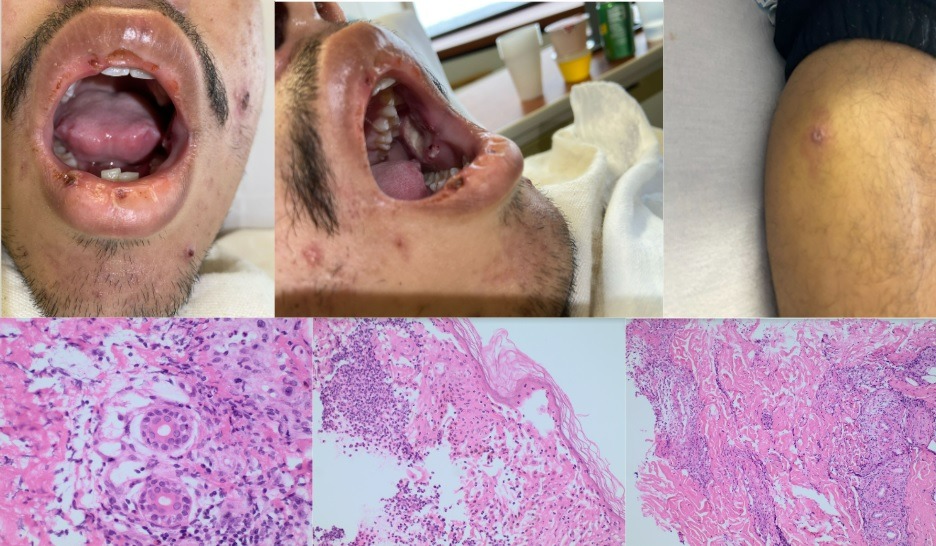
Figure: Top Row: Mucocutaneous findings in the Mouth and Left Lower Extremity
Bottom Row: Perivascular mixed inflammatory infiltrate primarily composed of neutrophils with a few eosinophils present with no evidence of vasculitis. The infiltrate is primarily limited to the dermis.
Disclosures:
Andreas Bub indicated no relevant financial relationships.
Jaspreet Suri indicated no relevant financial relationships.
Amr Sayed indicated no relevant financial relationships.
Andreas W. Bub, MD1, Jaspreet Suri, MD2, Amr Sayed, MD3. E0419 - Sweet Syndrome as One of the Manifesting Symptoms of Inflammatory Bowel Disease, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.