Luis M. Nieto, MD1, Steven Keilin, MD2 1WellStar Atlanta Medical Center, Atlanta, GA; 2Emory University School of Medicine, Atlanta, GA
Introduction: Colloid carcinoma (CC) of the pancreas is a rare variant of ductal adenocarcinoma (DAC) and represents 1% of pancreatic carcinomas. Nearly all CC cases develop from intrapapillary mucinous neoplasm (IPMN). CC is also recognized as a histological subtype of invasive IPMN and its differentiation from IPMN can be challenging. CC has been shown to have better overall survival than DAC but its recurrence rate has not been established. Also, the liver is the most common site of distant metastases in pancreatic invasive IPMN but its frequency has not been described in CC metastases. To our knowledge, no other case of pancreatic CC with multiple liver metastatic lesions and intrahepatic biliary duct (BD) recurrence has been reported.
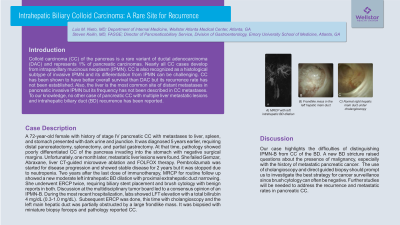
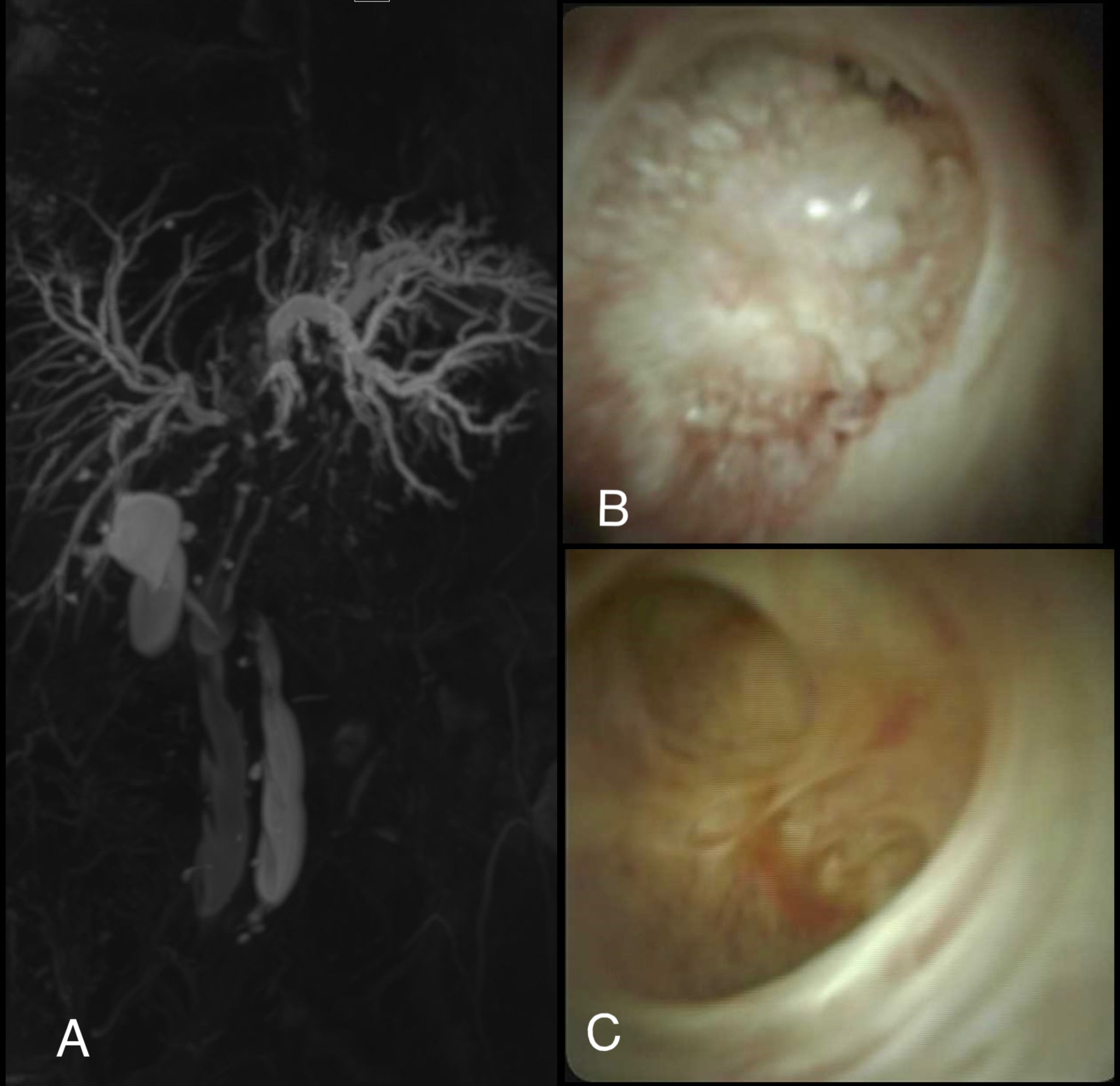
Case Description/Methods: A 72-year-old female with history of stage IV pancreatic CC with metastases to liver, spleen, and stomach presented with dark urine and jaundice. Diagnosed 5 years earlier, requiring distal pancreatectomy, splenectomy, and partial gastrectomy. At that time, pathology showed poorly differentiated CC of the pancreas invading into the stomach with negative surgical margins. Unfortunately, one month later, metastatic liver lesions were found. She failed Gemzar, Abraxane, liver CT-guided microwave ablation and FOLFOX therapy. Pembrolizumab was started for disease progression and showed stable disease for 2 years but it was stopped due to neutropenia. Two years after the last dose of immunotherapy, MRCP showed new moderate left intrahepatic duct dilation with left hepatic duct narrowing. She underwent ERCP twice, requiring biliary stent placement and brush cytology with benign results. Discussion at the multidisciplinary tumor board led to a consensus opinion of IPMN-B. During the most recent hospitalization, labs showed elevated liver function studies with a total bilirubin of 4 mg/dl. ERCP was done with cholangioscopy. The left main hepatic duct was partially obstructed by a large frondlike mass. It was biopsied and pathology reported as CC.
Discussion: Our case highlights the difficulties of distinguishing IPMN-B from CC of the BD. A new BD stricture raised questions about the presence of malignancy, especially with the history of metastatic pancreatic cancer. The cholangioscopy findings and the pathology report should make us investigate the best strategy for cancer surveillance since brush cytology can often be negative. Further studies will be needed to address the recurrence and metastatic rates in pancreatic CC.
Figure: Figure 1. A) MRCP with left intrahepatic BD dilation. B) Frondlike mass in the left hepatic main duct and C) normal right hepatic main duct under cholangioscopy
Disclosures:
Luis Nieto indicated no relevant financial relationships.
Steven Keilin indicated no relevant financial relationships.
Luis M. Nieto, MD1, Steven Keilin, MD2. E0030 - Intrahepatic Biliary Colloid Carcinoma: A Rare Site for Recurrence, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.