Wayne State University School of Medicine Rochester Hills, MI
Vatsal Khanna, MD, Bernadette Schmidt, MD, Ahmad Refai, MD, Joshua Gorney, MD, Issam A. Turk, MD Wayne State University School of Medicine, Rochester Hills, MI
Introduction: Pneumomediastinum (PM) is the presence of free air or gas within the mediastinum. It is often called spontaneous pneumomediastinum (SPM) in the absence of trauma or a clear secondary cause. The incidence of SPM is reported between 0.001% and 0.014% of hospitalized patients and is more commonly seen among young adult males.
We report a case of a 22-year-old male who developed SPM and pneumopericardium secondary to cannabinoid hyperemesis syndrome(CHS).
Case Description/Methods: We report a case of a 22-year-old male with a history of CHS who presented to the hospital with complaints of intractable nausea, vomiting, and generalized abdominal pain. The patient denied fever, chills, hematemesis, melena, or hematochezia. The patient has had similar episodes in the past treated with anti-emetics, not requiring hospital admission.
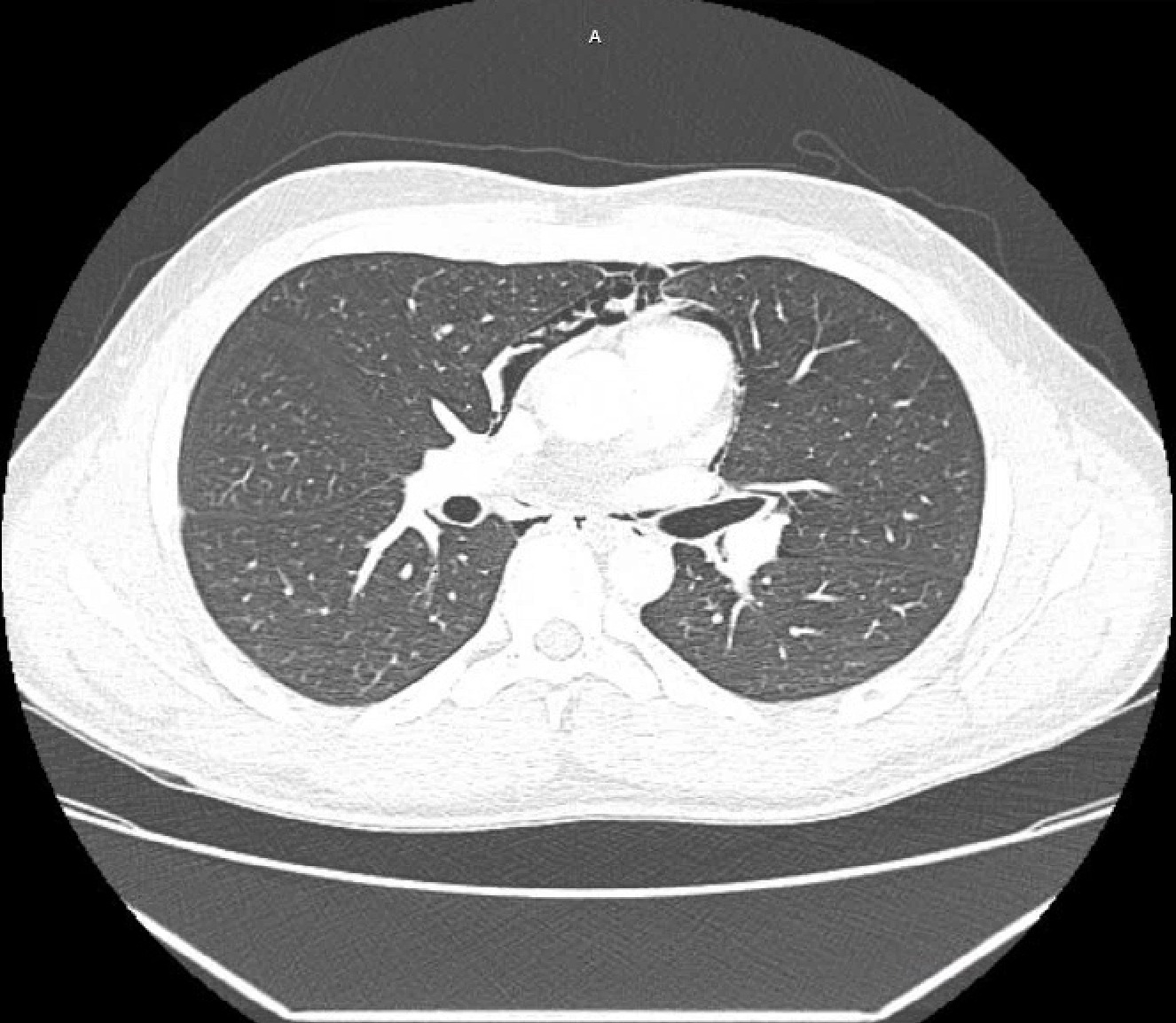
On admission, vitals were stable. Clinical laboratory results showed hypokalemia 3.3. Serum lipase was normal. Urinalysis was positive for cannabinoids. Electrocardiogram showed a normal sinus rhythm, no ST-T wave changes. Physical exam revealed a soft abdomen with diffuse abdominal tenderness and no signs of peritonitis, and the lungs were clear to auscultation. Subcutaneous crepitus was noted over the chest wall. A Computed Tomography (CT) of the abdomen with intravenous contrast showed no acute intra-abdominal pathology and the presence of PM. CT chest with intravenous and oral contrast showed extensive pneumomediastinum, a small pneumopericardium, and no extravasation of oral contrast. The patient was transferred to the intensive care unit for closer monitoring, and cardiothoracic surgery was consulted. The patient was treated conservatively, with complete recovery.
Discussion: SPM is a rare condition characterized by free air in the mediastinum not preceded by thoracic trauma. It consists of a triad of thoracic pain, subcutaneous emphysema, and dyspnea. In a retrospective review, Weiss et al. reported 14 cases of marijuana use associated with PM.
SPM results from alveolar rupture following an acute rise in intra-alveolar pressure. Cannabinoids have been used for their antiemetic properties, which are mediated by the cannabinoid receptor CB1. The stimulation of CB1 receptors can suppress gastric emptying in a dose-dependent manner, which may contribute to symptoms seen in CHS. In our case, PM may have resulted from the rupture of a subpleural bulla caused by forceful vomiting.
The treatment of SPM is usually conservative and surgery is reserved for unstable patients.
Figure: CT chest with contrast showing extensive pneumomediastinum
Disclosures:
Vatsal Khanna indicated no relevant financial relationships.
Bernadette Schmidt indicated no relevant financial relationships.
Ahmad Refai indicated no relevant financial relationships.
Joshua Gorney indicated no relevant financial relationships.
Issam Turk indicated no relevant financial relationships.
Vatsal Khanna, MD, Bernadette Schmidt, MD, Ahmad Refai, MD, Joshua Gorney, MD, Issam A. Turk, MD. C0698 - Spontaneous Pneumomediastinum and Pneumopericardium Secondary to Cannabinoid Hyperemesis Syndrome, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.