Tiberiu Moga, MD1, Andrew Bain, MD2, Kevin Robillard, MD2 1University at Buffalo, Buffalo, NY; 2Roswell Park Comprehensive Cancer Center, Buffalo, NY
Introduction: Gastrointestinal stromal tumors (GISTs) are the most common mesenchymal neoplasms of the stomach. GISTs can vary from small, asymptomatic lesions managed with surveillance to large lesions presenting with life-threatening complications, including gastrointestinal hemorrhage. Complications such cavitary lesions and luminal GI fistulas have been reported but are exceedingly rare.
Case Description/Methods: A 65 year-old woman developed mild, constant abdominal pain. Her past medical history includes HTN, GERD, COPD and 50 pack-year smoking history. One month after symptom onset, she was admitted to an outside hospital with upper GI bleed. EGD was reportedly normal at that time. She was readmitted one month later with recurrent anemia. CT scan showed a large gastric diverticulum or possible cavitary lesion. EGD was repeated and showed an opening to a large diverticulum or cavity distal to the gastroesophageal junction with ulcerated cavity wall. Pathology showed ulcerated gastric mucosa and granulation tissue with atypical spindle cells. Biopsies were negative for H. pylori.
She was then admitted to our hospital for severe anemia and work-up of suspected GIST. A third EGD showed a 2 cm fistula to a 10 cm necrotic cavity on the fundus and proximal greater curvature of the gastric body. Multiple biopsies of the cavity wall were taken. Biopsies were positive for spindle cell-type GIST (CD117+, CD34+, Cam 5.2-). She then had a feeding jejunostomy placed due to difficulty tolerating PO intake. She was treated with pantoprazole and imatinib and discharged with Medical Oncology and Surgery follow-up for resection.
Discussion: The most common site of origin for GISTs is the stomach. Radiographic appearance is variable and can include endoluminal, exophytic or dumbbell-shaped pattern and there is frequently necrosis. Other imaging findings include calcifications, cyst formation, cystic degeneration and rarely, cavitary lesions and fistulas. In fact, there are only 2 case reports in the last 10 years of GISTs presenting as a gastric fistula or a gastrobronchial fistula. CT findings including: hemorrhage, necrosis, calcifications, intralesional cavitation, cystic degeneration, size >10cm, irregular margins and heterogeneous enhancement all portend a poor prognosis. Enlarged feeding or draining vessels can predict relapse.
Our patient’s case shows that it is important to have a high index of suspicion for diagnosis of GIST, particularly in the setting of atypical presentation.
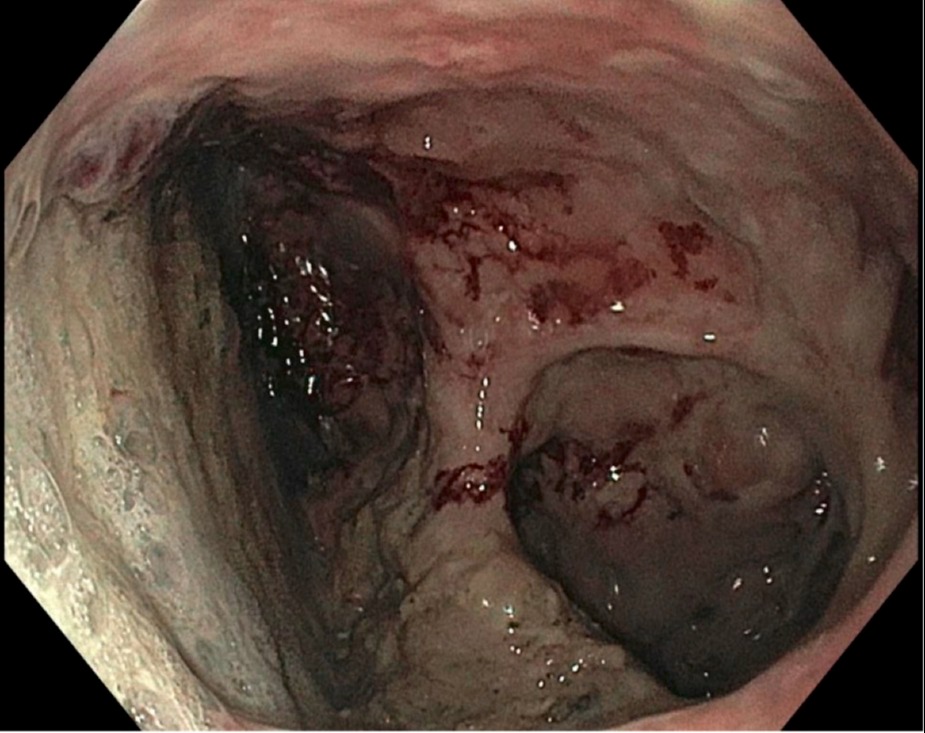
Figure: Figure 1: Upper GI endoscopy image of the interior of the GIST cavity.
Disclosures:
Tiberiu Moga indicated no relevant financial relationships.
Andrew Bain indicated no relevant financial relationships.
Kevin Robillard indicated no relevant financial relationships.
Tiberiu Moga, MD1, Andrew Bain, MD2, Kevin Robillard, MD2. C0702 - Gastrointestinal Stromal Tumor Presenting as a Fistulizing Cavitary Lesion, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.