Warren Alpert Medical School of Brown University Providence, RI
Aastha Chokshi, MD1, Lawrence Kogan, MD2, Yigit Baykara, MD3, Samir A. Shah, MD, FACG4 1Warren Alpert Medical School of Brown University , Providence, RI; 2Warren Alpert Medical School of Brown University, Providence, RI; 3The Warren Alpert Medical School of Brown University, Providence, RI; 4Warren Alpert Medical School / The Miriam Hospital, Providence, RI
Introduction: Xanthelasmas are benign lesions which are most commonly found on the skin but can also be found in the gastrointestinal (GI) tract. The stomach is the most common site within the GI tract for xanthelasmas with a prevalence of approximately 0.2-0.8%. Endoscopically, they appear as plaque like yellowish-white lesions, and on histology are characterized by foamy lipid laden histiocytes. Xanthelasmas are generally asymptomatic, and thus are usually incidental findings on esophagoduodenoscopies (EGDs) performed for variety of other indications. While they are themselves benign, gastric xanthelasmas are associated with H. pylori associated gastritis, chronic gastritis, as well as gastric dysplasia, emphasizing the need to identify and diagnose this otherwise rare condition.
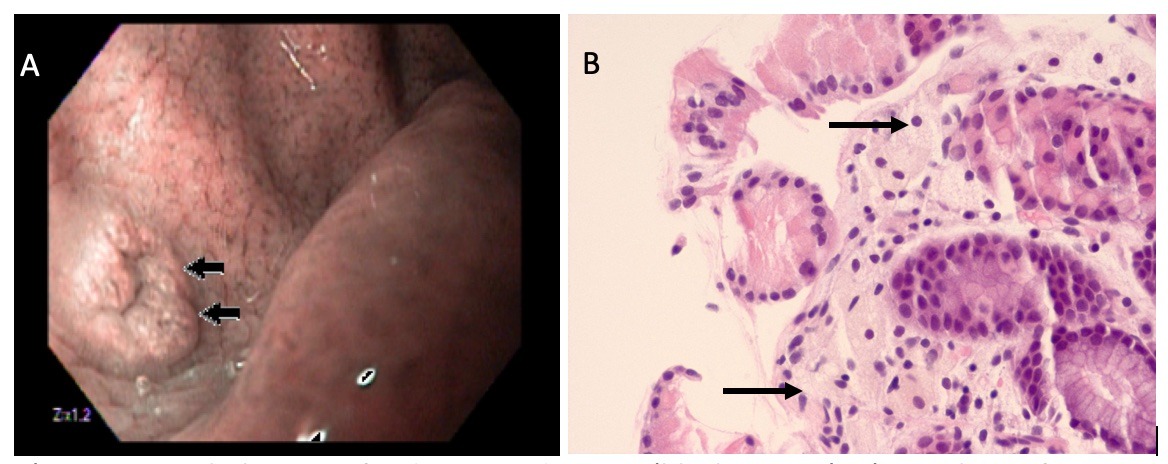
Case Description/Methods: We describe the case of a 43-year old male with medical history of hypertension and psoriatic arthritis who was referred for evaluation of dyspepsia and chronic heartburn. He was taking ibuprofen, celecoxib, hydrocodone-acetaminophen, losartan and was started on omeprazole prior to GI referral. Family history was notable for father with stomach cancer at age 48 and death at age 50. His vitals were within normal limits and his abdomen was soft, non-tender, non-distended. He underwent an upper endoscopy which showed a polypoid lesion in the fundus, but was otherwise unremarkable (Figure 1A). The polyp was biopsied and was suggestive of a xanthelasma, without evidence of metaplasia or dysplasia (Figure 1B). Given improvements in his symptoms, he was told to decrease the omeprazole dose and avoid NSAIDs. Follow up EGD at 6 months and 7 years showed no evidence of recurrence and screening colonoscopy at age 50 also showed no signs in the lower GI tract.
Discussion: Gastrointestinal xanthelasmas are rare, and tend to be more commonly found in women. They are usually incidental endoscopic findings and are generally benign. However, they can be associated with pre-cancerous states including gastritis and gastric dysplasia. A prior study has shown that the presence of a gastric xanthelasma was independently associated with gastric cancer with an odds ratio of 6.19. The location of a xanthelasma in the upper region of the stomach was also significantly associated with gastric cancer. This highlights the importance of identification of these lesions on endoscopy with subsequent biopsy for identification and closer monitoring.
Figure: Figure 1. A) Gastric xanthelasma in fundus on endoscopy (black arrows). B) Histology of gastric xanthelasma showing foamy lipid laden macrophages (black arrow).
Disclosures:
Aastha Chokshi indicated no relevant financial relationships.
Lawrence Kogan indicated no relevant financial relationships.
Yigit Baykara indicated no relevant financial relationships.
Samir Shah indicated no relevant financial relationships.
Aastha Chokshi, MD1, Lawrence Kogan, MD2, Yigit Baykara, MD3, Samir A. Shah, MD, FACG4. C0297 - Gastric Xanthelasma: A Rare Endoscopic Finding, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.