Andy Silva-Santisteban, MD1, Neal Mehta, MD2, Roberto Trasolini, MD1, James Stone, MD2, Douglas K. Pleskow, MD1 1Beth Israel Deaconess Medical Center, Boston, MA; 2BIDMC, Boston, MA
Introduction: Bouveret syndrome is a rare condition characterized by the impaction of a gallstone in the stomach or duodenum via a fistulous tract resulting in gastric outlet obstruction. This condition generally requires surgery to remove the impacted stone. However, for patients who are unable to undergo surgery, laser lithotripsy can be an alternative therapy. Here, we present an interesting case of a patient with recurrent gallstone ileus successfully treated by endoscopic Holmium laser lithotripsy
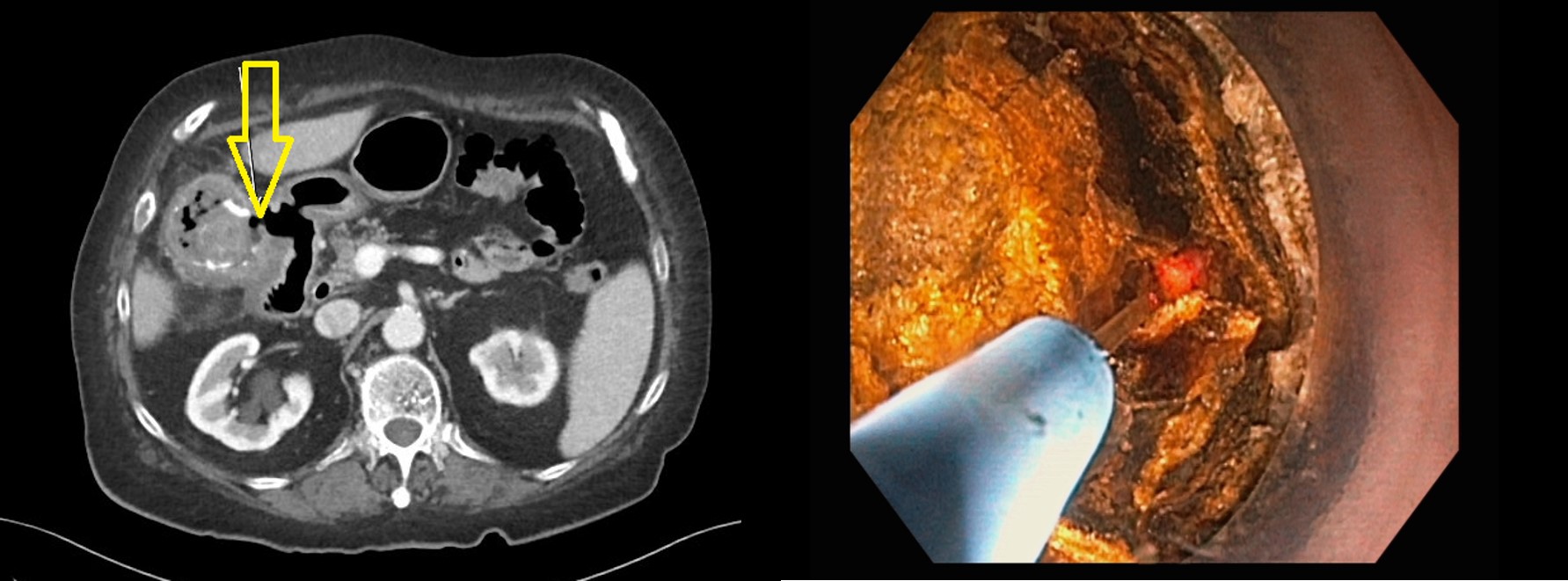
Case Description/Methods: A frail 79-year-old woman with chronic cholecystitis presented with right upper quadrant abdominal pain. Abdominal computed tomography (CT) scan demonstrated emphysematous calculous cholecystitis, a cholecystoduodenal fistula and a 30 mm gallstone lodged in the terminal ileum. She emergently underwent an ileocecal resection and partial right colectomy, confirming the diagnosis of gallstone ileus and a small bowel perforation. 10 days post-surgically, the patient again developed nausea, vomiting, and right upper quadrant pain. CT imaging re-demonstrated a 40 mm gallstone within the gallbladder fossa, Surgical options were limited due to a friable duodenum and inflammation of the cholecystoduodenal fistula. After a multidisciplinary discussion, endoscopic therapy was planned.
Endoscopically, a large gallstone measuring about 40 mm was into the duodenal bulb eroding into the duodenum consistent with the known fistula. Holmium laser lithotripsy was used to fragment the stone. Due to the size of the gallstone, the procedure was performed in two sessions. During the first session, the stone was successfully fractured into smaller fragments. In the subsequent session, the remaining gallstone measuring about 28 mm was fragmented until the fistula tract was cleared. The larger gallstone fragments were removed using a roth net and a stone retrieval basket. Full resolution of the Bouveret syndrome was achieved. No immediate or delayed complications were noted. The patient is now doing well 3 months post-procedurally.
Discussion: Although surgery is often required for definitive therapy of Bouveret syndrome , endoscopic management remains a feasible option in select cases with appropriate expertise. Here, we present a case of successful endoscopic therapy utilizing Holmium laser lithotripsy in a high-risk patient for Bouveret syndrome. Although utilizing this technique is lengthy and requires advanced endoscopic expertise, provides a great benefit due to its minimal tissue injury and safety.
Figure: Image: A) Cholecystoduedenal fistula on CT scan, B) Holmium laser lithotripsy for Bouveret syndrome
Disclosures:
Andy Silva-Santisteban indicated no relevant financial relationships.
Neal Mehta indicated no relevant financial relationships.
Roberto Trasolini indicated no relevant financial relationships.
James Stone indicated no relevant financial relationships.
Douglas Pleskow: Boston scientifics – Consultant.
Andy Silva-Santisteban, MD1, Neal Mehta, MD2, Roberto Trasolini, MD1, James Stone, MD2, Douglas K. Pleskow, MD1. B0189 - Endoscopic Holmium Laser Lithotripsy for Therapy of Bouveret Syndrome, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.