Bing Chen, MD1, Bolun Liu, MD2, Katherine Sun, MD, PhD3, Christopher Cordeiro, MD3, Howard Chung, MD3, Chetan Virmani, MD3, Beishi Zheng, MD4, Alexander Shapsis, MD5 1New York University School of Medicine, New York, NY; 2Mayo Clinic Health System, Mankato, MN; 3NYU Grossman School of Medicine, New York, NY; 4Woodhull Medical and Mental Health Center, Brooklyn, NY; 5Atlantic Gastroenterology, Brooklyn, NY
Introduction: Signet ring cell carcinoma accounts for about one percent of all colorectal cancers. It is an aggressive subtype of adenocarcinomas with the tendency for intramural spread and peritoneal carcinomatosis. Here, we reported a middle-aged male with circumferential colonic stenosis and inconclusive histology, found to have stage 4 colorectal signet ring cell carcinoma (SRCC).
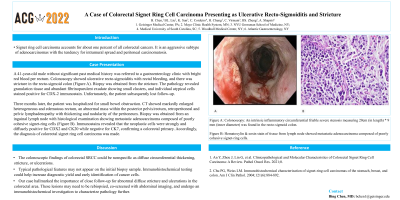
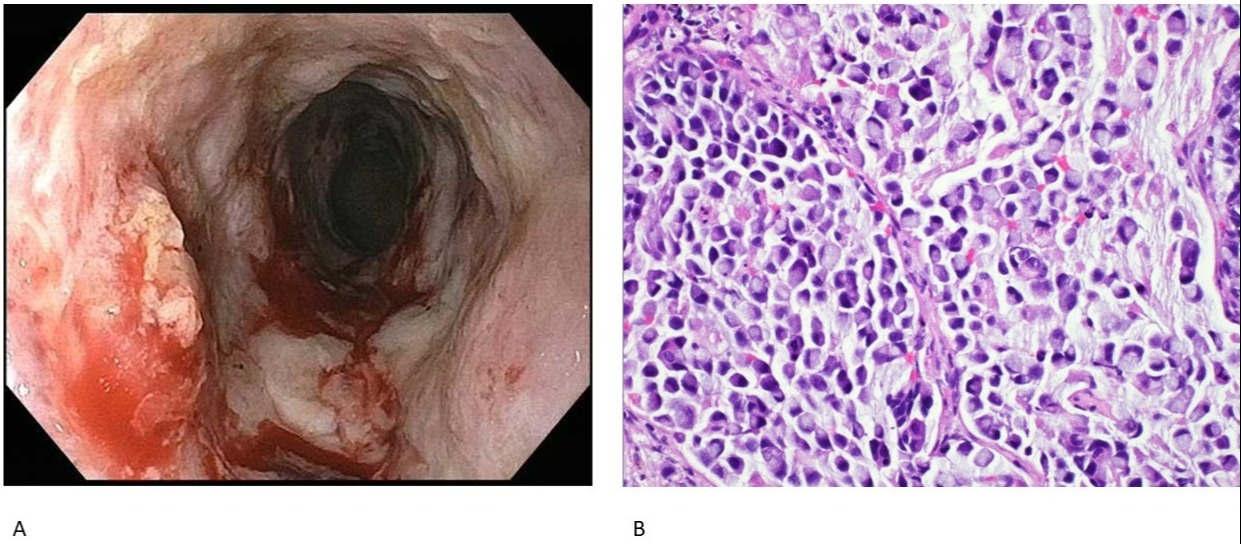
Case Description/Methods: A 41-year-old male without significant past medical history was referred to a gastroenterology clinic with bright red blood per rectum. Colonoscopy showed ulcerative recto-sigmoiditis with rectal bleeding, and there was stricture in the rectum, in the recto-sigmoid colon, and from anus to descending colon (Figure A). Biopsy was obtained from the stricture. The pathology revealed granulation tissue and abundant fibrinopurulent exudate showing small clusters, and individual atypical cells stained positive for CDX-2 immunostain. Unfortunately, the patient subsequently lost follow-up.
Three months later, the patient was hospitalized for small bowel obstruction. CT showed markedly enlarged heterogeneous and edematous rectum, an abnormal mass within the posterior pelvis/rectum, retroperitoneal and pelvic lymphadenopathy with thickening and nodularity of the peritoneum. Biopsy was obtained from an inguinal lymph node with histological examination showing metastatic adenocarcinoma composed of poorly cohesive signet-ring cells (Figure B). Immunostains revealed that the neoplastic cells were strongly and diffusely positive for CDX2 and CK20 while negative for CK7, confirming a colorectal primary. Accordingly, the diagnosis of colorectal signet ring cell carcinoma was made.
Discussion: The colonoscopic findings of colorectal SRCC could be nonspecific as diffuse circumferential thickening, stricture, or ulcerations. Typical pathological features may not appear on the initial biopsy sample. Immunohistochemical testing could help increase diagnostic yield and early identification of cancer cells. Our case hallmarked the importance of close follow-up for abnormal diffuse stricture and ulcerations in the colorectal area. These lesions may need to be rebiopsied, co-screened with abdominal imaging, and undergo an immunohistochemical investigation to characterize pathology further.
Figure: Figure A: Colonoscopy: An intrinsic inflammatory circumferential fibrosis friable severe stenosis measuring 20cm (in length) * 9 mm (inner diameter) was found in the rectum, in the recto-sigmoid colon, and from anus to descending colon.
Figure B: Hematoxylin & eosin stain of tissue from lymph node showed metastatic adenocarcinoma composed of poorly cohesive signet-ring cells.
Disclosures:
Bing Chen indicated no relevant financial relationships.
Bolun Liu indicated no relevant financial relationships.
Katherine Sun indicated no relevant financial relationships.
Christopher Cordeiro indicated no relevant financial relationships.
Howard Chung indicated no relevant financial relationships.
Chetan Virmani indicated no relevant financial relationships.
Beishi Zheng indicated no relevant financial relationships.
Alexander Shapsis: Abbvie – Speaker. Gilliad – Speaker.
Bing Chen, MD1, Bolun Liu, MD2, Katherine Sun, MD, PhD3, Christopher Cordeiro, MD3, Howard Chung, MD3, Chetan Virmani, MD3, Beishi Zheng, MD4, Alexander Shapsis, MD5. A0110 - A Case of Colorectal Signet Ring Cell Carcinoma Presenting as Ulcerative Recto-Sigmoiditis and Stricture, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.