Praneeth Kudaravalli, MD1, Kwabena O. Adu-Gyamfi, MBChB2, Kenneth J. Vega, MD, FACG3, John Erikson L. Yap, MD3 1Augusta University Medical Center, Augusta, GA; 2Medical College of Georgia - Augusta University, Augusta, GA; 3Augusta University Medical College of Georiga, Augusta, GA
Introduction: Cystic fibrosis (CF) is regarded as a lung disease as the primary morbidity and mortality are secondary to pulmonary related complications. However, gastrointestinal diseases are an increasingly important cause of morbidity in these patients due to expanding survival. These complications require special management consideration as they are unique to CF patients, requiring appropriate diagnosis and treatment. Our case illustrates distal intestinal obstruction syndrome (DIOS) which is a CF specific gastrointestinal complication.
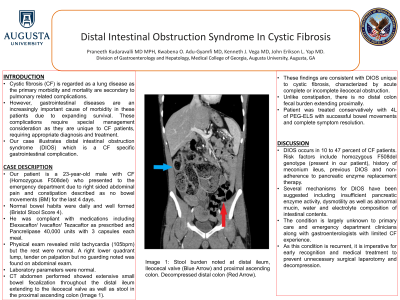
Case Description/Methods: Our patient is a 23-year-old male with CF (Homozygous F508del) who presented to the emergency department due to right sided abdominal pain and constipation described as no bowel movements (BM) for the last 4 days. Normal bowel habits were daily and well formed (Bristol Stool Score 4). He was compliant with medications including Elexacaftor/ Ivacaftor/ Tezacaftor as prescribed and Pancrelipase 40,000 units with 3 capsules each meal. Physical exam revealed mild tachycardia (105bpm) but the rest were normal. A right lower quadrant lump, tender on palpation but no guarding noted was found on abdominal exam. Laboratory parameters were normal. CT abdomen performed showed extensive small bowel fecalization throughout the distal ileum extending to the ileocecal valve as well as stool in the proximal ascending colon. These findings are consistent with DIOS unique to cystic fibrosis, characterized by acute complete or incomplete ileocecal obstruction. Unlike constipation, there is no distal colon fecal burden extending proximally. Patient was treated conservatively with 4L of PEG-ELS with successful bowel movements and complete symptom resolution.
Discussion: DIOS occurs in 10 to 47 percent of CF patients. Risk factors include homozygous F508del genotype (present in our patient), history of meconium ileus, previous DIOS and non-adherence to pancreatic enzyme replacement therapy. Several mechanisms for DIOS have been suggested including insufficient pancreatic enzyme activity, dysmotility as well as abnormal mucin, water and electrolyte composition of intestinal contents. The condition is largely unknown to primary care and emergency department clinicians along with gastroenterologists with limited CF experience. As this condition is recurrent, it is imperative for early recognition and medical treatment to prevent unnecessary surgical laparotomy and decompression.
Figure: Image A – Stool burden noted proximal at distal ileum, Ileocecal valve (Blue Arrow) and proximal ascending colon. Decompressed distal colon (Red Arrow).
Disclosures:
Praneeth Kudaravalli indicated no relevant financial relationships.
Kwabena Adu-Gyamfi indicated no relevant financial relationships.
Kenneth Vega indicated no relevant financial relationships.
John Erikson Yap indicated no relevant financial relationships.
Praneeth Kudaravalli, MD1, Kwabena O. Adu-Gyamfi, MBChB2, Kenneth J. Vega, MD, FACG3, John Erikson L. Yap, MD3. A0116 - Distal Intestinal Obstruction Syndrome in Cystic Fibrosis, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.