
Category: Infections in Immunocompromised Individuals
Poster Session: Infections in Immunocompromised Individuals

Will Garner
Infectious Diseases Fellow
University of Pittsburgh Medical Center
Pittsburgh, Pennsylvania
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.
Palash Samanta
Dr
UPMC
Pittsburgh, Pennsylvania
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.
Kathleen Dorritie
Assistant Professor of Medicine
University of Pittsburgh Medical Center, University of Pittsburgh, Hillman Cancer Center
Pittsburgh, Pennsylvania
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.
Alison Sehgal
Assistant Professor of Medicine
University of Pittsburgh Medical Center, University of Pittsburgh, Hillman Cancer Center
Pittsburgh, Pennsylvania
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.
Denise Winfield
Nurse Practitioner
University of Pittsburgh Medical Center, Hillman Cancer Center
Pittsburgh, Pennsylvania
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.
Mounzer Agha
Director of the Mario Lemieux Center for Blood Cancers, Associate Professor of Medicine
University of Pittsburgh Medical Center, University of Pittsburgh, Hillman Cancer Center
Pittsburgh, Pennsylvania
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.
Robert Boudreau
Core Director for Biostatistics, Center for Aging and Population Health, Assistant Professor
University of Pittsburgh
Pittsburgh, Pennsylvania
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.
M. Hong T. Nguyen
Professorof Medicine
University of Pittsburgh School of Medicine
Pittsburgh, Pennsylvania
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.

Ghady Haidar
Assistant Professor of Medicine
University of Pittsburgh School of Medicine
Pittsburgh, PA
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.
CAR T -cell therapy (CTT) is a novel treatment for B-cell cancers. CTT patients (pt) are at risk of infection due to neutropenia, cytokine release syndrome (CRS), and CAR T-cell related encephalopathy syndrome (CRES), which are treated with steroids and tocilizumab (anti-IL-6). This is a single-center study evaluating the risk factors for infection after CTT.
Methods:
A retrospective review was conducted of 60 consecutive CTT recipients between 7/17/17 and 9/5/19. Data was collected from 6 months (mo) pre- and at least 6 mo post-CTT. Data was censored for death, additional chemotherapy, or loss to follow up. Cox proportional hazard and Poisson regression were used.
Results:
Median age was 66 (23-84) years; 48% (29) were female. The most common cancer was non-Hodgkin lymphoma (89%, 54). 25% (15) had a prior stem cell transplant (SCT). 73% (44) and 45% (27) of pts developed CRS and CRES, respectively. 43% (26) received steroids; 65% (39) received tocilizumab. In the 6 mo pre-CTT, 39 infections occurred in 45% (27) of pts. 103 infections occurred in 66% (40) after CTT; 33 (55%) had an infection within 6 mo. Infections were bacterial (52%; 54/103), viral (30%; 37/103), fungal (10%; 10/103), mycobacterial (1%; 1/103), protozoal (1%; 1/103). Cumulative incidence of infection in the first 6 mo are shown in Fig 1. All-cause and infection-related mortality were 32% (19) and 15% (9), respectively. Mortality among pts with fungal infections was 20% (2/10). Infection density was 1.28 and 0.58 infections per 100 pt-days between days 0-30 and 30-89, respectively. Factors associated with infection post CTT were number (no.) of infections in the 6 mo prior to infusion (HR 1.62, CI [1.1-2.38]; p=0.015), no. of lines of therapy in the 6 mo pre-CTT (HR 1.52, CI [1.01-2.27]; p=0.04), prior allogeneic SCT (HR 5.96, CI [1.34-26.47]; p=0.019), and no. of tocilizumab doses. Grade 1 CRS and grade 2 CRES were risk factors between days 0-30 and 0-180, respectively (HR 4.67, CI [1.02 -21.4], p = 0.047; HR 2.48, CI [1.17-5.23], p = 0.02).Fig 1: Cumulative Incidence of Infection 6 Months Post CAR T-cell Therapy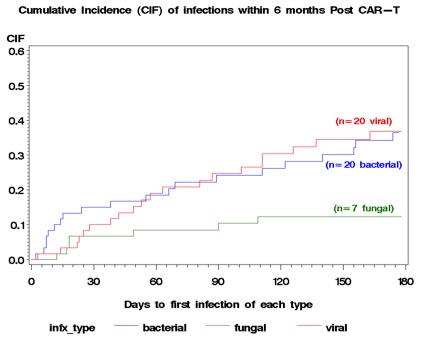
Conclusion:
Infections after CTT are common. Infection before CTT was associated with risk of infection after CTT. Pt selection may ameliorate this risk. Mortality due to fungal infections was high. Randomized-controlled trials of antifungal prophylaxis in high-risk pts are needed.
