
Category: Respiratory Infections - Viral
Poster Session: Respiratory Infections - Viral


Zaid Haddadin
Postdoctoral Research Fellow
Vanderbilt University Medical Center; Division of Pediatric Infectious Diseases
Nashville, Tennessee
Disclosure: CDC (Grant/Research Support, Research Grant or Support)Quidel Corporation (Grant/Research Support, Research Grant or Support)sanofi pasteur (Grant/Research Support, Research Grant or Support)

Danielle A. Rankin
Doctoral Candidate in Epidemiology
Vanderbilt University Medical Center
Nashville, Tennessee
Disclosure: Sanofi Pasteur (Grant/Research Support, Research Grant or Support)
loren lipworth
Research Professor
Division of Epidemiology - 104370
Nashville, Tennessee
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.
Jon Fryzek
Principal Epidemiologist Practice Director
EpidStrategies, A Division of ToxStrategies, Inc.
Rockville, MD
Disclosure: EpidStrategies (Employee)

Mina Suh
Senior Epidemiologist
Epidstrategies
Mission Viejo, California
Disclosure: EpidStrategies (Employee)

Donald S. Shepard
Professor
Brandeis University
Waltham, Massachusetts
Disclosure: Sanofi Pasteur (Grant/Research Support)
Rendie McHenry
Research Asst III
Vanderbilt University Medical Center; Division of Pediatric Infectious Diseases
Nashville, Tennessee
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.
Rebekkah Varjabedian
Clin/Tran Research Coord II
Vanderbilt University Medical Center; Division of Pediatric Infectious Diseases
Nashville, Tennessee
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.

Kailee N. Fernandez
Clin/Tran Research Coordinator I
Vanderbilt University Medical Center; Division of Pediatric Infectious Diseases
Nashville, Tennessee
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.

Christopher B. Nelson
Associate Vice President
Sanofi
Swiftwater, Pennsylvania
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.

Natasha B. Halasa
Craig Weaver Professor of Pediatrics
Vanderbilt University Medical Center
Nashville, TN
Disclosure: Genentech (Other Financial or Material Support, I receive an honorarium for lectures - it's a education grant, supported by genetech)Karius (Consultant)Moderna (Consultant)Quidel (Grant/Research Support, Research Grant or Support)Sanofi (Grant/Research Support, Research Grant or Support)
Viral acute respiratory infections (ARI) continues to be a significant cause of healthcare visits in young children. We evaluated the clinical presentation and disease severity of common respiratory viruses associated with medically attended ARI in infants.
Methods:
We conducted a prospective viral surveillance study in Davidson County, TN. Infants under one year with fever and/or respiratory symptoms were enrolled from the outpatient (OP), emergency department (ED), or inpatient (IP) settings from 12/16/2019 through 4/30/2020. Nasal swabs were collected and tested for common viral pathogens using Luminex® NxTAG Respiratory Pathogen Panel. Demographic and clinical characteristics were collected through parent/guardian interviews and medical chart abstractions.
Results:
In total, 364 participants were enrolled, and 361 (99%) had nasal swabs collected and tested. Overall, mean age was 6±3.3 months, 50% were female, 45% White, and 27% Hispanic. Of the 295 (82%) virus-positive specimens; the three most common viruses were rhinovirus/enterovirus (RV/EV), respiratory syncytial virus (RSV), and influenza (flu) [124, 101, and 44, respectively]. Compared to virus-negative infants, virus-positive infants were more likely to have more severe ARI symptoms and to be admitted to the intensive care unit (Table 1). Compared to other virus-positive infants: RV/EV-positive infants were more likely to be White, attend daycare, but less likely to present with respiratory distress, or require oxygen or admission; flu-positive infants were older and more likely to have systemic symptoms rather than ARI symptoms, and RSV-positive infants were more likely to present with respiratory distress, receive oxygen and be hospitalized (Table 1).Table 1. Demographic and Clinical Characteristics of Study Subjects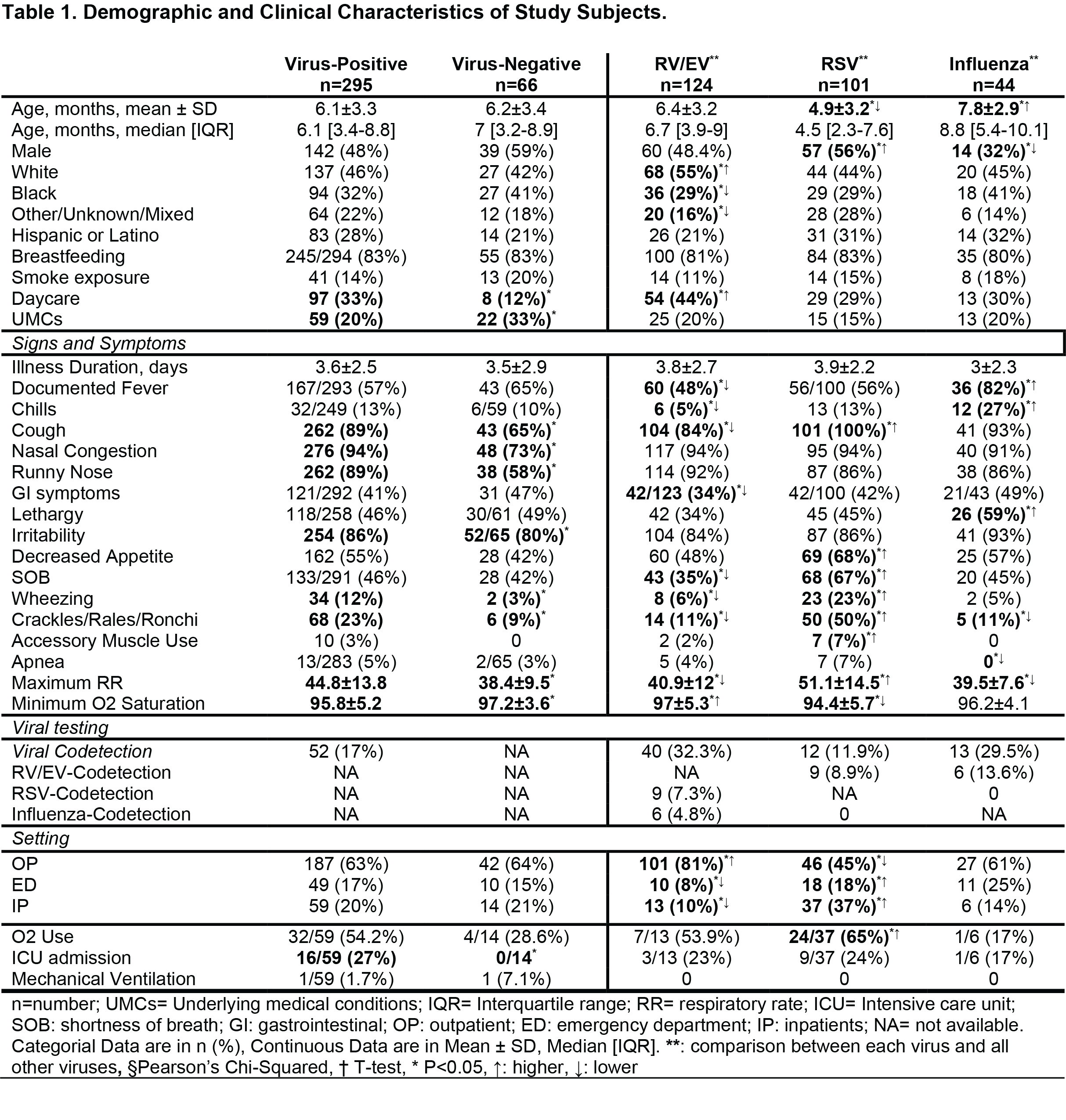
Conclusion:
The majority of ARI in infants are due to respiratory viruses, with RSV, RV/EV, and flu accounting for over three-quarters of these viruses. The clinical presentations and disease severity differed across the clinical settings and the three main viruses, with RSV being most severe. To decrease the burden of medically attended viral ARI, preventive measures (i.e., developing new vaccines and antivirals), refining current vaccination strategies, and infection control measures are needed.
