
Category: Global Health
Poster Session: Global Health


Zaid Haddadin
Postdoctoral Research Fellow
Vanderbilt University Medical Center; Division of Pediatric Infectious Diseases
Nashville, Tennessee
Disclosure: CDC (Grant/Research Support, Research Grant or Support)Quidel Corporation (Grant/Research Support, Research Grant or Support)sanofi pasteur (Grant/Research Support, Research Grant or Support)

Danielle A. Rankin
Doctoral Candidate in Epidemiology
Vanderbilt University Medical Center
Nashville, Tennessee
Disclosure: Sanofi Pasteur (Grant/Research Support, Research Grant or Support)
Ahmad Yanis
Research Assistant
Vanderbilt University Medical Center; Division of Pediatric Infectious Diseases
Nashville, Tennessee
Disclosure: Quidel Corporation (Grant/Research Support)
Yanal Shawareb
Research Assistant
Vanderbilt University Medical Center; Division of Pediatric Infectious Diseases
Nashville, Tennessee
Disclosure: Quidel (Grant/Research Support)Quidel (Grant/Research Support, Research Grant or Support, Sanofi)
Olla Hamdan
Research Assistant
Vanderbilt University Medical Center; Division of Pediatric Infectious Diseases
Nashville, Tennessee
Disclosure: Quidel (Grant/Research Support, Research Grant or Support)
Malek Saada
Resident Physician
Al Bashir Hospital
amman, 'Amman, Jordan
Disclosure: Quidel Corporation (Grant/Research Support, Research Grant or Support)
Sara Hilal
Resident Physician
Al Bashir Hospital
amman, 'Amman, Jordan
Disclosure: Quidel Corporation (Grant/Research Support, Research Grant or Support)
Ahmad Alhajajra
Attending Physician
Al Bashir Hospital
amman, 'Amman, Jordan
Disclosure: Quidel Corporation (Grant/Research Support, Research Grant or Support)
Basima Marar
Professor of Pediatrics
Al-Bashir Hospital
Amman, Amman, Jordan
Disclosure: Quidel Corporation (Grant/Research Support, Research Grant or Support)
Najwa Khuri-Bulos
Distinguished Professor
University of Jordan
Amman, 'Amman, Jordan
Disclosure: Quidel Corporation (Grant/Research Support, Research Grant or Support)
Respiratory syncytial virus (RSV) is the leading cause of acute respiratory infections (ARI) hospitalizations in young children and is associated with increased severity compared to other viruses. The aim of this study was to evaluate the utilization of a rapid RSV diagnostic test and clinical characteristics and disease severity of children who were hospitalized during one respiratory season in Amman, Jordan.
Methods:
Children less than two years hospitalized with fever and/or respiratory symptoms were recruited at Al-Bashir Government Hospital from January 8, 2020, to March 17, 2020. Nasal swabs were collected and tested by Sofia-2 RSV Fluorescent Immunoassay. Demographic information and clinical history were obtained through parental interviews. A validated severity score was used to assess disease severity, and the treating physician prospectively collected the necessary information to calculate the score at admission. Disease severity was categorized based on the total score into 0-5 mild, 6-9 moderate, and ≥ 10 severe. Molecular testing and medical chart reviews are still in process.
Results:
A total of 532 subjects were enrolled, and nasal swabs were collected and tested from 458 (86%) of enrollees. The most common admission diagnoses were pneumonia (25%), bronchopneumonia (21%), bronchiolitis (19%) and sepsis (17%). Demographic and clinical characteristics are included in Table 1. Overall, 276 (60%) subjects were RSV-positive. The most common admission diagnoses were pneumonia (33%), sepsis (25%), bronchiolitis (24%) and bronchopneumonia (24%). Compared to RSV-negative children, RSV-positive children were younger (Table 1), and more likely to present with cough, nasal congestion, and appetite loss (Figure 1). There were no differences in severity score or direct intensive care unit admission between the two groups (Table 1). Table 1. Demographic and Clinical Characteristics of the Study Cohort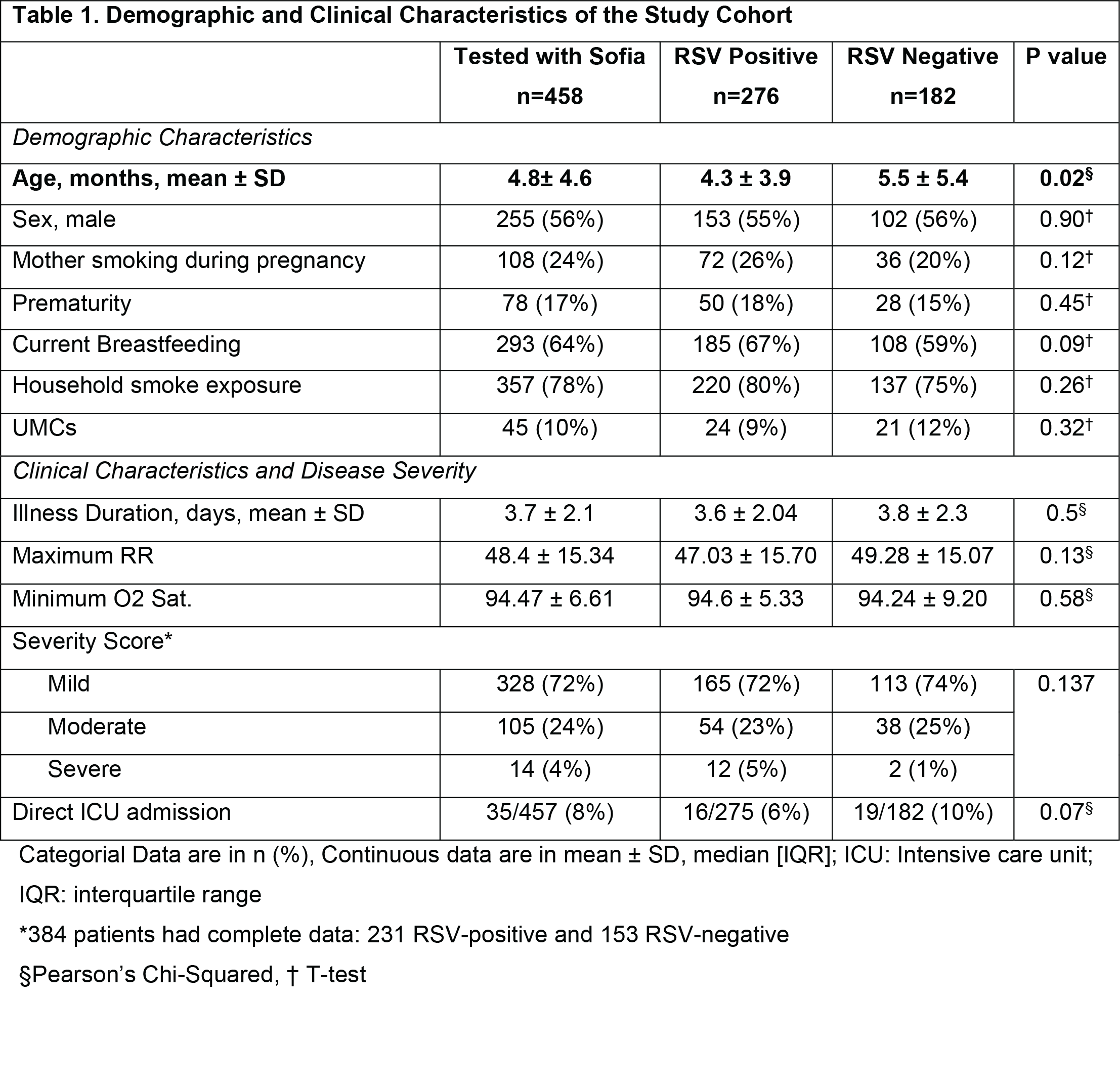 Figure 1. Symptom Distribution in RSV-Positive and RSV-Negative Subjects
Figure 1. Symptom Distribution in RSV-Positive and RSV-Negative Subjects.png)
Conclusion:
Nearly 2/3 of children enrolled were RSV-positive via rapid diagnostic testing. The majority of RSV-ARI admissions were classified as mild. Further analysis of other clinical parameters, including oxygen use, intravenous fluids administration and length of stay, and molecular testing are needed to support these findings and further evaluate the utility of rapid diagnostic testing.
