
Category: HAI: C. difficile
Poster Session: HAI: C. difficile

Raghavendra Tirupathi
Medical Director
Keystone Health
Chambersberg, Pennsylvania
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.
Ruth Freshman
Director
Wellspan Health
Chambersburg, Pennsylvania
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.
Norma Montoy
Infection Preventionist
wellspan health
Chambersburg, Pennsylvania
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.
Melissa Gross
Pharmacist
wellspan health
Chambersburg, Pennsylvania
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.
An estimated 15% of hospitalized patients are asymptomatic carriers of C. diff. Inappropriate testing can lead to over diagnosis, treatment, isolation & substantial financial penalties. Ours is a rural 310 bed hospital with nurse driven C. diff test ordering protocol. Due to inadvertent test ordering, we had an uptick in the HO-CDI incidence with rates as high as 0.94 per 1000 patient days in 2017. In order to streamline testing, we initiated an infection preventionist(IP) led diagnostic stewardship program which was implemented in two phases in 2017-2019
Methods:
The phase 1 involved daily review by IPs regarding the legitimacy of PCR order for minimum 3 loose stools in 24 hours, use of laxatives, presence of symptoms.There were concerns nationally that then CDI risk adjustment model from NHSN in 2017 does not optimally account for the impact of specific CDI testing methods used by individual hospitals on CDI SIRs. Hence, in Jan 2018 NHSN’s MDRO/CDI Protocol stated “Results of the final test that are placed in the patient’s medical record should be used to determine whether event meets the CDI LabID defn”.This led to phase 2 in mar 2019 which involved two step testing which started with C diff PCR assay with positive test reflexed to the toxin A/B assay.
Results:
During the first phase, and a full year of the protocol in 2018, the number of completed PCR tests decreased to 626 (compared to 940 PCR tests in 2016) with an 34% decrease. In the year following implementation of the Diagnostic Stewardship, HO CDI decreased from 60 in 2017 to 43 events in 2018 with a reduction of 28%. Subsequently, HO CDI further decreased in 2019 to 28 with a reduction of 35%. Since the start of the project in 2017, HO CDI have decreased 54% in total. The reduction in 314 C diff PCR tests in the first year[2017-2018] led to a savings of $8300 in lab supplies. No readmissions with C difficile infection documented within 30 days on patients who did not meet the criterion for testing. Significant decrease in the usage of C difficile antibiotics. After the start of the two step test, we have seen a precipitous drop in our HO-CDI rates to less than 0.3 per 1000 pt days by the end of 2019. Quarterly comparison of HO CDI incidence for 2017-2020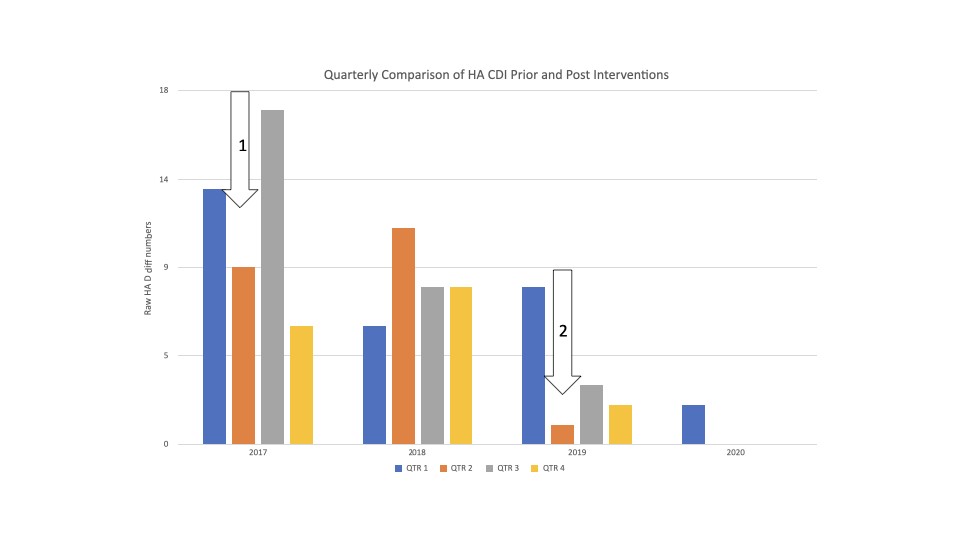 HO CDI incidence before and following phase 1 and phase 2 interventions
HO CDI incidence before and following phase 1 and phase 2 interventions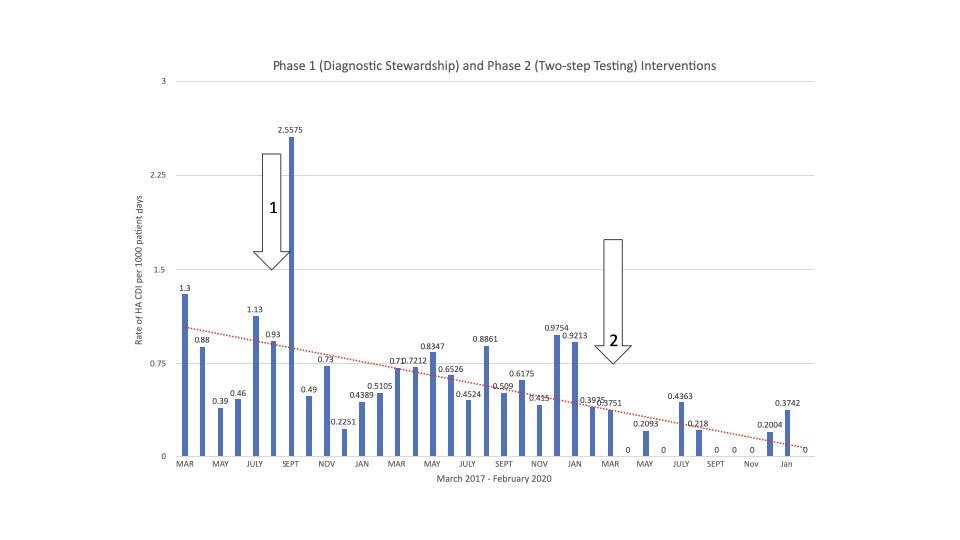 C. difficile antibiotic use trends during intervention period
C. difficile antibiotic use trends during intervention period
Conclusion:
IP run diagnostic stewardship programs with two step tests are highly successful in streamlining testing and in discriminating infection from colonization
